.png)


.svg)
.svg)

Refined Mid‑Face Contouring: Buccal Fat Removal Explained
News
/
April 22, 2026
Buccal Fat Removal: Sculpting Your Mid‑Face for a Slimmer Profile
Refined Mid‑Face Contouring: Buccal Fat Removal Explained

Body contouring has revolutionized the way we think about self-care and aesthetic transformations. It’s more than just a cosmetic procedure—it’s a path to enhanced confidence and self-expression.
Introduction to Buccal Fat Removal
Buccal fat removal, also called cheek reduction or buccal lipectomy, is performed with a small intra‑oral incision along the upper gum line to access the deep buccal fat pads located between the masseter and buccinator muscles. Under local anesthesia with optional IV sedation (or general anesthesia when combined with other procedures), the surgeon gently excises 2–5 ml of fat per side, closes the mucosal incision with dissolvable sutures, and the patient returns home the same day. The results are permanent because the removed fat cells do not regenerate.
Patients choose this approach to achieve a slimmer, more V‑shaped mid‑face, enhanced cheekbone definition, and a harmonious facial contour without visible external scars. The procedure is brief (30‑60 minutes), involves minimal downtime, and can be safely combined with chin grafting, fillers, or a mid‑face lift for comprehensive facial rejuvenation when performed by a board‑certified facial plastic surgeon.
Anatomy, Candidate Selection, and Cultural Perspectives
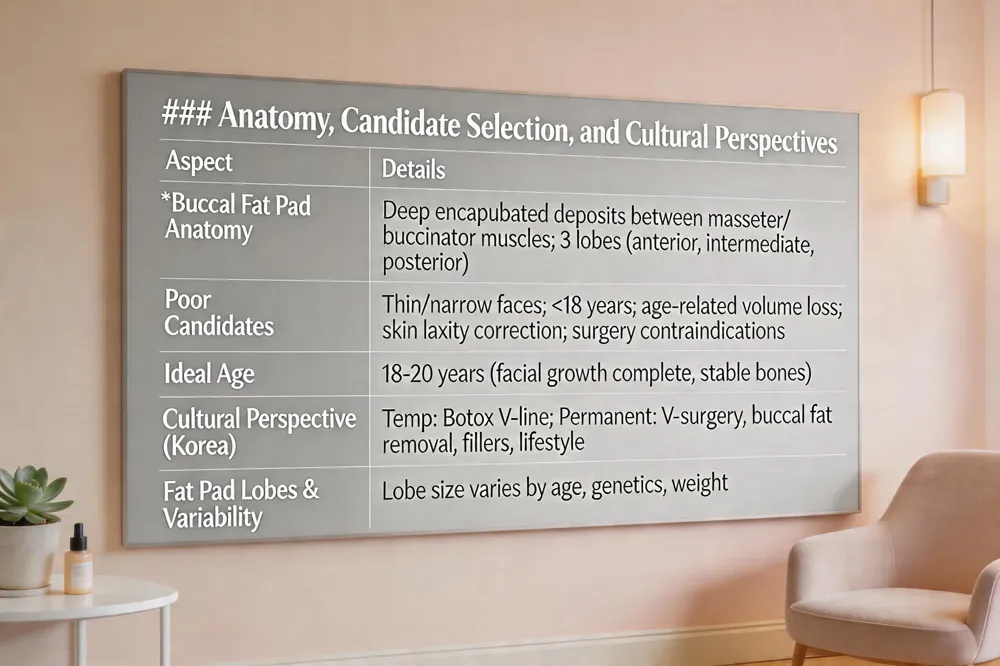 Buccal fat pads are deep, encapsulated deposits situated between the masseter and buccinator muscles, beneath the cheekbones and above the mandibular ramus. They contribute to mid‑face fullness and protect neurovascular structures.
Who is not a good candidate? Patients with naturally thin or narrow faces, those still undergoing facial growth (typically under 18 years), older individuals with age‑related volume loss, and anyone seeking to correct skin laxity rather than excess buccal fat are poor candidates. Significant medical contraindications to oral surgery or anesthesia also exclude patients.
Ideal age for the procedure? Most surgeons recommend waiting until facial growth is complete, around 18‑20 years, when bone structure is stable and natural fat reduction can be assessed. This timing helps avoid over‑reduction in younger patients and prevents a gaunt appearance in older adults.
Cultural perspective – Korean face‑slimming methods: In Korea, non‑surgical approaches like masseter Botox are common for a temporary V‑line effect. More permanent options include V‑line jaw surgery, chin augmentation, buccal fat removal, and facial liposuction. Thread lifts and dermal fillers further define contours, while lifestyle measures (skincare, facial massage, low‑sodium diet) support results.
Buccal fat pads: These pads are three‑lobed structures (anterior, intermediate, posterior) with extensions that lie between facial muscles and the skin, varying in size by age, genetics, and weight.
Procedure, Effects, and Financial Considerations
Cost Overview
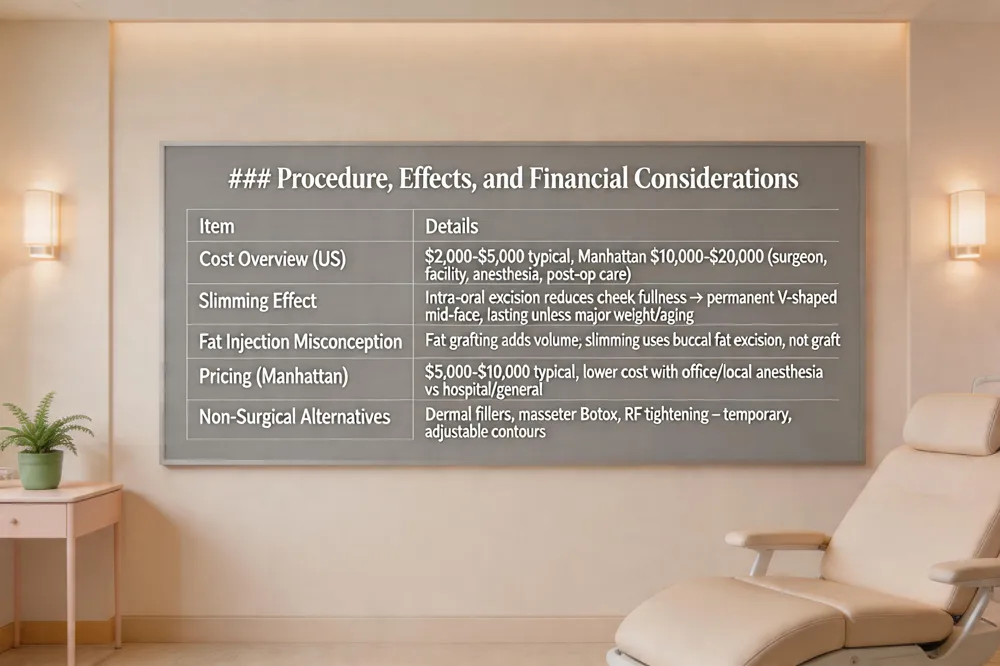
In the United States, buccal fat removal typically costs $2,000‑$5,000 in most markets, but in high‑cost cities such as Manhattan the total fee can rise to $10,000‑$20,000 when surgeon honorarium, facility, anesthesia, and post‑operative care are included. Prices vary with surgeon experience, office‑based versus hospital setting, and anesthetic method. Most insurers consider the procedure elective, so patients often use financing or payment plans.
Slimming Effect
Removing the buccal fat pad via an intra‑oral incision reduces cheek fullness and creates a narrower, V‑shaped mid‑face. Because the excised fat cells do not regenerate, the slimming effect is permanent, though natural aging and weight changes can alter overall facial volume. Ideal candidates are healthy adults with stable weight and a naturally rounded mid‑face; the procedure is usually performed after facial maturity (age 18‑20).
Fat Injection Misconception
Buccal fat removal is rarely performed; instead, dermal fillers are employed to add volume. For patients seeking a slimmer look, surgeons favor surgical excision of excess buccal fat rather than fat grafting, as the latter adds rather than removes volume.
Before & After Gallery
Private galleries at practices such as Premier Cosmetic Surgery & Medspa (Arcadia, CA) and Dr. Loeb’s Manhattan office display subtle reductions in cheek width and enhanced jawline definition while preserving natural facial harmony.
Pricing Details
A typical Manhattan fee ranges $5,000‑$10,000, reflecting surgeon expertise, anesthesia type, and facility fees. Office‑based procedures under local anesthesia are generally less expensive than hospital‑based surgeries with general anesthesia.
Non‑Surgical Alternatives
For those wishing to avoid permanent fat loss, options include injectable dermal fillers, Botox for masseter reduction, and radio‑frequency skin tightening. These approaches provide temporary contour changes and can be adjusted over time, unlike the permanent nature of buccal fat removal.
Recovery Timeline, Side Effects, and Long‑Term Follow‑Up
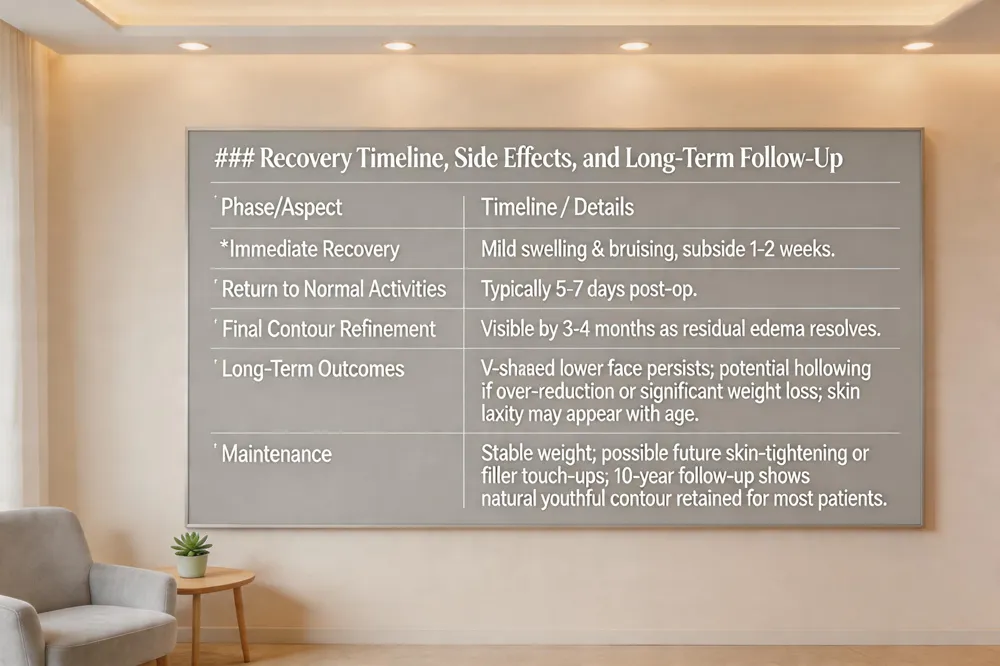 Buccal fat removal produces a lasting V‑shaped lower face because the excised fat cells do not regenerate. Ideal patients—typically over 18–20 years old with stable weight—enjoy enhanced cheek‑bone definition for many years. However, excessive removal or later significant weight loss can leave the cheeks overly hollow, especially in naturally narrow faces. Age‑related skin laxity may also accentuate a sunken look, so surgeons often recommend maintenance of stable weight and, if needed, future skin‑tightening or filler procedures to preserve harmony.
Recovery photo timelines show mild swelling and bruising that subside within one to two weeks, with most patients returning to normal activities in 5–7 days. Final contour refinement becomes evident by three to four months as residual edema resolves. Clinics such as Premier Cosmetic Surgery & Medspa and Dr. Loeb’s practice provide patients with visual milestones to set realistic expectations.
Ten‑year follow‑up data indicate that the majority of patients retain a natural, youthful contour. A gradual loss of facial volume can occur with aging, but it is usually manageable with non‑surgical touch‑ups like dermal fillers. Ongoing monitoring ensures any asymmetry or over‑reduction is addressed promptly, preserving a balanced facial aesthetic over the long term.
Combining Procedures: Mid‑Face Lift, Cheek Lift, and Perioral Refinement
 A mid‑face lift elevates the cheek and nasolabial areas, restoring a youthful V‑shaped contour, but it does not treat the eyelids; periorbital rejuvenation typically requires a separate blepharoplasty. Before‑and‑after photographs consistently show lifted cheek projection, softened nasolabial folds, and a smoother mid‑face while preserving natural expression. In major metropolitan markets such as New York City, the comprehensive cost of a mid‑face lift ranges from $12,000 to $20,000, encompassing surgeon fees, anesthesia, and facility charges.
For patients seeking a non‑surgical cheek lift, options include dermal fillers, thread lifts, or radio‑frequency skin tightening. These modalities provide temporary contour improvement without incisions, making them suitable for those not ready for operative intervention.
Perioral mounds—often the result of excess fat, laxity, or volume loss around the mouth—can be addressed through a combination of buccal fat removal, targeted fillers, and resurfacing techniques. Buccal fat excision reduces deep mid‑cheek fullness, while fillers restore lost volume in the perioral region, and skin resurfacing improves texture, achieving balanced facial harmony.
When planning a comprehensive facial rejuvenation, surgeons frequently combine a mid‑face lift with buccal fat removal, cheek lift, or chin augmentation to achieve a harmonious, sculpted appearance. Careful pre‑operative analysis, including photographic documentation and, when available, 3‑D imaging, ensures appropriate fat removal volume and minimizes risks such as asymmetry, nerve injury, or over‑resection. Post‑operative care generally involves a soft‑food diet for the first 24–48 hours, oral hygiene with prescribed rinses, and avoidance of strenuous facial expressions for one to two weeks. Most patients resume normal activities within five to seven days, with final aesthetic results becoming evident after three to six months as swelling subsides.
Celebrity Cases and Complication Management
 Celebrity Experiences: Several high‑profile figures, including model Megan Fox and actress Hilary Duff, have publicly disclosed undergoing buccal fat removal to achieve a slimmer, more defined cheek contour. Their disclosures have helped normalize the procedure and illustrate that it can be performed safely in an outpatient setting under local anesthesia with intra‑oral incisions, leaving no external scars.
Potential Complications: While buccal fat removal is generally well‑tolerated, complications can arise. Reported issues include asymmetry, over‑reduction that creates an unnaturally hollow appearance, infection, hematoma, temporary numbness, and rare facial nerve injury. Proper patient selection—healthy adults with stable weight and no naturally narrow facial structure—combined with a board‑certified facial plastic surgeon skilled in precise intra‑oral dissection, minimizes these risks. Post‑operative care such as a soft diet, oral hygiene, and monitoring for signs of infection further supports optimal outcomes.
Patient Gallery and Long‑Term Satisfaction
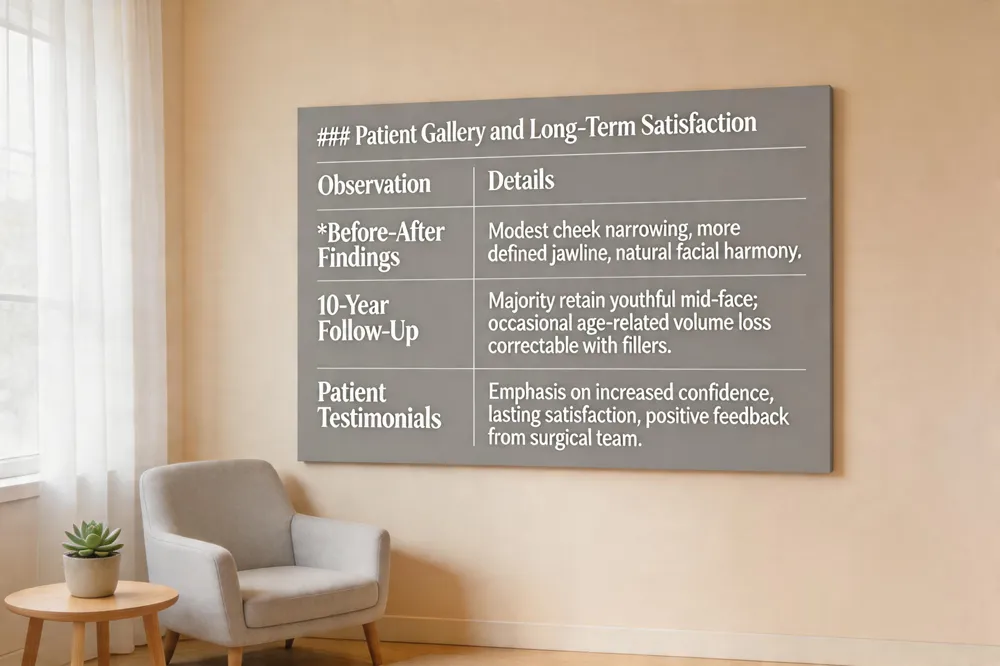 Our patient gallery displays before‑and‑after photos that illustrate a modest narrowing of the cheeks and a more defined jawline while preserving natural harmony. Ten‑year follow‑up data show most individuals keep a youthful, sculpted mid‑face; occasional age‑related volume loss can be corrected with fillers. Testimonials highlight confidence and lasting satisfaction and continued positive feedback from our team.
Conclusion – A Balanced, Personalized Approach to Mid‑Face Sculpting
Key Takeaways: Buccal fat removal thins the mid‑face by excising buccal fat pads through an intra‑oral incision, leaving no external scar. Results are permanent because the fat cells do not regenerate, although aging and weight changes can alter contour. Ideal candidates are healthy adults with full cheeks and expectations; thin‑boned or older patients may be unsuitable.
Importance of Expert Guidance: A board‑certified facial plastic surgeon must evaluate facial anatomy, skin elasticity, and skeletal proportions before deciding how much fat to remove. Precise technique protects the facial nerve, salivary ducts, and Stenson’s duct, reducing risks of asymmetry, infection, or numbness. Counseling sets goals and care.
Future Aesthetic Planning: Since buccal fat does not regrow, patients should anticipate loss and consider fillers, chin augmentation, or a mid‑face lift to preserve balance. Ongoing monitoring and a maintenance plan help maintain appearance.
Introduction to Buccal Fat Removal
Buccal fat removal, also called cheek reduction or buccal lipectomy, is performed with a small intra‑oral incision along the upper gum line to access the deep buccal fat pads located between the masseter and buccinator muscles. Under local anesthesia with optional IV sedation (or general anesthesia when combined with other procedures), the surgeon gently excises 2–5 ml of fat per side, closes the mucosal incision with dissolvable sutures, and the patient returns home the same day. The results are permanent because the removed fat cells do not regenerate.
Patients choose this approach to achieve a slimmer, more V‑shaped mid‑face, enhanced cheekbone definition, and a harmonious facial contour without visible external scars. The procedure is brief (30‑60 minutes), involves minimal downtime, and can be safely combined with chin grafting, fillers, or a mid‑face lift for comprehensive facial rejuvenation when performed by a board‑certified facial plastic surgeon.
Anatomy, Candidate Selection, and Cultural Perspectives
 Buccal fat pads are deep, encapsulated deposits situated between the masseter and buccinator muscles, beneath the cheekbones and above the mandibular ramus. They contribute to mid‑face fullness and protect neurovascular structures.
Who is not a good candidate? Patients with naturally thin or narrow faces, those still undergoing facial growth (typically under 18 years), older individuals with age‑related volume loss, and anyone seeking to correct skin laxity rather than excess buccal fat are poor candidates. Significant medical contraindications to oral surgery or anesthesia also exclude patients.
Ideal age for the procedure? Most surgeons recommend waiting until facial growth is complete, around 18‑20 years, when bone structure is stable and natural fat reduction can be assessed. This timing helps avoid over‑reduction in younger patients and prevents a gaunt appearance in older adults.
Cultural perspective – Korean face‑slimming methods: In Korea, non‑surgical approaches like masseter Botox are common for a temporary V‑line effect. More permanent options include V‑line jaw surgery, chin augmentation, buccal fat removal, and facial liposuction. Thread lifts and dermal fillers further define contours, while lifestyle measures (skincare, facial massage, low‑sodium diet) support results.
Buccal fat pads: These pads are three‑lobed structures (anterior, intermediate, posterior) with extensions that lie between facial muscles and the skin, varying in size by age, genetics, and weight.
Procedure, Effects, and Financial Considerations

Cost Overview
In the United States, buccal fat removal typically costs $2,000‑$5,000 in most markets, but in high‑cost cities such as Manhattan the total fee can rise to $10,000‑$20,000 when surgeon honorarium, facility, anesthesia, and post‑operative care are included. Prices vary with surgeon experience, office‑based versus hospital setting, and anesthetic method. Most insurers consider the procedure elective, so patients often use financing or payment plans.
Slimming Effect
Removing the buccal fat pad via an intra‑oral incision reduces cheek fullness and creates a narrower, V‑shaped mid‑face. Because the excised fat cells do not regenerate, the slimming effect is permanent, though natural aging and weight changes can alter overall facial volume. Ideal candidates are healthy adults with stable weight and a naturally rounded mid‑face; the procedure is usually performed after facial maturity (age 18‑20).
Fat Injection Misconception
Buccal fat removal is rarely performed; instead, dermal fillers are employed to add volume. For patients seeking a slimmer look, surgeons favor surgical excision of excess buccal fat rather than fat grafting, as the latter adds rather than removes volume.
Before & After Gallery
Private galleries at practices such as Premier Cosmetic Surgery & Medspa (Arcadia, CA) and Dr. Loeb’s Manhattan office display subtle reductions in cheek width and enhanced jawline definition while preserving natural facial harmony.
Pricing Details
A typical Manhattan fee ranges $5,000‑$10,000, reflecting surgeon expertise, anesthesia type, and facility fees. Office‑based procedures under local anesthesia are generally less expensive than hospital‑based surgeries with general anesthesia.
Non‑Surgical Alternatives
For those wishing to avoid permanent fat loss, options include injectable dermal fillers, Botox for masseter reduction, and radio‑frequency skin tightening. These approaches provide temporary contour changes and can be adjusted over time, unlike the permanent nature of buccal fat removal.
Recovery Timeline, Side Effects, and Long‑Term Follow‑Up
 Buccal fat removal produces a lasting V‑shaped lower face because the excised fat cells do not regenerate. Ideal patients—typically over 18–20 years old with stable weight—enjoy enhanced cheek‑bone definition for many years. However, excessive removal or later significant weight loss can leave the cheeks overly hollow, especially in naturally narrow faces. Age‑related skin laxity may also accentuate a sunken look, so surgeons often recommend maintenance of stable weight and, if needed, future skin‑tightening or filler procedures to preserve harmony.
Recovery photo timelines show mild swelling and bruising that subside within one to two weeks, with most patients returning to normal activities in 5–7 days. Final contour refinement becomes evident by three to four months as residual edema resolves. Clinics such as Premier Cosmetic Surgery & Medspa and Dr. Loeb’s practice provide patients with visual milestones to set realistic expectations.
Ten‑year follow‑up data indicate that the majority of patients retain a natural, youthful contour. A gradual loss of facial volume can occur with aging, but it is usually manageable with non‑surgical touch‑ups like dermal fillers. Ongoing monitoring ensures any asymmetry or over‑reduction is addressed promptly, preserving a balanced facial aesthetic over the long term.
Combining Procedures: Mid‑Face Lift, Cheek Lift, and Perioral Refinement
 A mid‑face lift elevates the cheek and nasolabial areas, restoring a youthful V‑shaped contour, but it does not treat the eyelids; periorbital rejuvenation typically requires a separate blepharoplasty. Before‑and‑after photographs consistently show lifted cheek projection, softened nasolabial folds, and a smoother mid‑face while preserving natural expression. In major metropolitan markets such as New York City, the comprehensive cost of a mid‑face lift ranges from $12,000 to $20,000, encompassing surgeon fees, anesthesia, and facility charges.
For patients seeking a non‑surgical cheek lift, options include dermal fillers, thread lifts, or radio‑frequency skin tightening. These modalities provide temporary contour improvement without incisions, making them suitable for those not ready for operative intervention.
Perioral mounds—often the result of excess fat, laxity, or volume loss around the mouth—can be addressed through a combination of buccal fat removal, targeted fillers, and resurfacing techniques. Buccal fat excision reduces deep mid‑cheek fullness, while fillers restore lost volume in the perioral region, and skin resurfacing improves texture, achieving balanced facial harmony.
When planning a comprehensive facial rejuvenation, surgeons frequently combine a mid‑face lift with buccal fat removal, cheek lift, or chin augmentation to achieve a harmonious, sculpted appearance. Careful pre‑operative analysis, including photographic documentation and, when available, 3‑D imaging, ensures appropriate fat removal volume and minimizes risks such as asymmetry, nerve injury, or over‑resection. Post‑operative care generally involves a soft‑food diet for the first 24–48 hours, oral hygiene with prescribed rinses, and avoidance of strenuous facial expressions for one to two weeks. Most patients resume normal activities within five to seven days, with final aesthetic results becoming evident after three to six months as swelling subsides.
Celebrity Cases and Complication Management
 Celebrity Experiences: Several high‑profile figures, including model Megan Fox and actress Hilary Duff, have publicly disclosed undergoing buccal fat removal to achieve a slimmer, more defined cheek contour. Their disclosures have helped normalize the procedure and illustrate that it can be performed safely in an outpatient setting under local anesthesia with intra‑oral incisions, leaving no external scars.
Potential Complications: While buccal fat removal is generally well‑tolerated, complications can arise. Reported issues include asymmetry, over‑reduction that creates an unnaturally hollow appearance, infection, hematoma, temporary numbness, and rare facial nerve injury. Proper patient selection—healthy adults with stable weight and no naturally narrow facial structure—combined with a board‑certified facial plastic surgeon skilled in precise intra‑oral dissection, minimizes these risks. Post‑operative care such as a soft diet, oral hygiene, and monitoring for signs of infection further supports optimal outcomes.
Patient Gallery and Long‑Term Satisfaction
 Our patient gallery displays before‑and‑after photos that illustrate a modest narrowing of the cheeks and a more defined jawline while preserving natural harmony. Ten‑year follow‑up data show most individuals keep a youthful, sculpted mid‑face; occasional age‑related volume loss can be corrected with fillers. Testimonials highlight confidence and lasting satisfaction and continued positive feedback from our team.
Conclusion – A Balanced, Personalized Approach to Mid‑Face Sculpting
Key Takeaways: Buccal fat removal thins the mid‑face by excising buccal fat pads through an intra‑oral incision, leaving no external scar. Results are permanent because the fat cells do not regenerate, although aging and weight changes can alter contour. Ideal candidates are healthy adults with full cheeks and expectations; thin‑boned or older patients may be unsuitable.
Importance of Expert Guidance: A board‑certified facial plastic surgeon must evaluate facial anatomy, skin elasticity, and skeletal proportions before deciding how much fat to remove. Precise technique protects the facial nerve, salivary ducts, and Stenson’s duct, reducing risks of asymmetry, infection, or numbness. Counseling sets goals and care.
Future Aesthetic Planning: Since buccal fat does not regrow, patients should anticipate loss and consider fillers, chin augmentation, or a mid‑face lift to preserve balance. Ongoing monitoring and a maintenance plan help maintain appearance.
Heading
Introduction to Buccal Fat Removal
Buccal fat removal, also called cheek reduction or buccal lipectomy, is performed with a small intra‑oral incision along the upper gum line to access the deep buccal fat pads located between the masseter and buccinator muscles. Under local anesthesia with optional IV sedation (or general anesthesia when combined with other procedures), the surgeon gently excises 2–5 ml of fat per side, closes the mucosal incision with dissolvable sutures, and the patient returns home the same day. The results are permanent because the removed fat cells do not regenerate.
Patients choose this approach to achieve a slimmer, more V‑shaped mid‑face, enhanced cheekbone definition, and a harmonious facial contour without visible external scars. The procedure is brief (30‑60 minutes), involves minimal downtime, and can be safely combined with chin grafting, fillers, or a mid‑face lift for comprehensive facial rejuvenation when performed by a board‑certified facial plastic surgeon.
Anatomy, Candidate Selection, and Cultural Perspectives
 Buccal fat pads are deep, encapsulated deposits situated between the masseter and buccinator muscles, beneath the cheekbones and above the mandibular ramus. They contribute to mid‑face fullness and protect neurovascular structures.
Who is not a good candidate? Patients with naturally thin or narrow faces, those still undergoing facial growth (typically under 18 years), older individuals with age‑related volume loss, and anyone seeking to correct skin laxity rather than excess buccal fat are poor candidates. Significant medical contraindications to oral surgery or anesthesia also exclude patients.
Ideal age for the procedure? Most surgeons recommend waiting until facial growth is complete, around 18‑20 years, when bone structure is stable and natural fat reduction can be assessed. This timing helps avoid over‑reduction in younger patients and prevents a gaunt appearance in older adults.
Cultural perspective – Korean face‑slimming methods: In Korea, non‑surgical approaches like masseter Botox are common for a temporary V‑line effect. More permanent options include V‑line jaw surgery, chin augmentation, buccal fat removal, and facial liposuction. Thread lifts and dermal fillers further define contours, while lifestyle measures (skincare, facial massage, low‑sodium diet) support results.
Buccal fat pads: These pads are three‑lobed structures (anterior, intermediate, posterior) with extensions that lie between facial muscles and the skin, varying in size by age, genetics, and weight.
Procedure, Effects, and Financial Considerations

Cost Overview
In the United States, buccal fat removal typically costs $2,000‑$5,000 in most markets, but in high‑cost cities such as Manhattan the total fee can rise to $10,000‑$20,000 when surgeon honorarium, facility, anesthesia, and post‑operative care are included. Prices vary with surgeon experience, office‑based versus hospital setting, and anesthetic method. Most insurers consider the procedure elective, so patients often use financing or payment plans.
Slimming Effect
Removing the buccal fat pad via an intra‑oral incision reduces cheek fullness and creates a narrower, V‑shaped mid‑face. Because the excised fat cells do not regenerate, the slimming effect is permanent, though natural aging and weight changes can alter overall facial volume. Ideal candidates are healthy adults with stable weight and a naturally rounded mid‑face; the procedure is usually performed after facial maturity (age 18‑20).
Fat Injection Misconception
Buccal fat removal is rarely performed; instead, dermal fillers are employed to add volume. For patients seeking a slimmer look, surgeons favor surgical excision of excess buccal fat rather than fat grafting, as the latter adds rather than removes volume.
Before & After Gallery
Private galleries at practices such as Premier Cosmetic Surgery & Medspa (Arcadia, CA) and Dr. Loeb’s Manhattan office display subtle reductions in cheek width and enhanced jawline definition while preserving natural facial harmony.
Pricing Details
A typical Manhattan fee ranges $5,000‑$10,000, reflecting surgeon expertise, anesthesia type, and facility fees. Office‑based procedures under local anesthesia are generally less expensive than hospital‑based surgeries with general anesthesia.
Non‑Surgical Alternatives
For those wishing to avoid permanent fat loss, options include injectable dermal fillers, Botox for masseter reduction, and radio‑frequency skin tightening. These approaches provide temporary contour changes and can be adjusted over time, unlike the permanent nature of buccal fat removal.
Recovery Timeline, Side Effects, and Long‑Term Follow‑Up
 Buccal fat removal produces a lasting V‑shaped lower face because the excised fat cells do not regenerate. Ideal patients—typically over 18–20 years old with stable weight—enjoy enhanced cheek‑bone definition for many years. However, excessive removal or later significant weight loss can leave the cheeks overly hollow, especially in naturally narrow faces. Age‑related skin laxity may also accentuate a sunken look, so surgeons often recommend maintenance of stable weight and, if needed, future skin‑tightening or filler procedures to preserve harmony.
Recovery photo timelines show mild swelling and bruising that subside within one to two weeks, with most patients returning to normal activities in 5–7 days. Final contour refinement becomes evident by three to four months as residual edema resolves. Clinics such as Premier Cosmetic Surgery & Medspa and Dr. Loeb’s practice provide patients with visual milestones to set realistic expectations.
Ten‑year follow‑up data indicate that the majority of patients retain a natural, youthful contour. A gradual loss of facial volume can occur with aging, but it is usually manageable with non‑surgical touch‑ups like dermal fillers. Ongoing monitoring ensures any asymmetry or over‑reduction is addressed promptly, preserving a balanced facial aesthetic over the long term.
Combining Procedures: Mid‑Face Lift, Cheek Lift, and Perioral Refinement
 A mid‑face lift elevates the cheek and nasolabial areas, restoring a youthful V‑shaped contour, but it does not treat the eyelids; periorbital rejuvenation typically requires a separate blepharoplasty. Before‑and‑after photographs consistently show lifted cheek projection, softened nasolabial folds, and a smoother mid‑face while preserving natural expression. In major metropolitan markets such as New York City, the comprehensive cost of a mid‑face lift ranges from $12,000 to $20,000, encompassing surgeon fees, anesthesia, and facility charges.
For patients seeking a non‑surgical cheek lift, options include dermal fillers, thread lifts, or radio‑frequency skin tightening. These modalities provide temporary contour improvement without incisions, making them suitable for those not ready for operative intervention.
Perioral mounds—often the result of excess fat, laxity, or volume loss around the mouth—can be addressed through a combination of buccal fat removal, targeted fillers, and resurfacing techniques. Buccal fat excision reduces deep mid‑cheek fullness, while fillers restore lost volume in the perioral region, and skin resurfacing improves texture, achieving balanced facial harmony.
When planning a comprehensive facial rejuvenation, surgeons frequently combine a mid‑face lift with buccal fat removal, cheek lift, or chin augmentation to achieve a harmonious, sculpted appearance. Careful pre‑operative analysis, including photographic documentation and, when available, 3‑D imaging, ensures appropriate fat removal volume and minimizes risks such as asymmetry, nerve injury, or over‑resection. Post‑operative care generally involves a soft‑food diet for the first 24–48 hours, oral hygiene with prescribed rinses, and avoidance of strenuous facial expressions for one to two weeks. Most patients resume normal activities within five to seven days, with final aesthetic results becoming evident after three to six months as swelling subsides.
Celebrity Cases and Complication Management
 Celebrity Experiences: Several high‑profile figures, including model Megan Fox and actress Hilary Duff, have publicly disclosed undergoing buccal fat removal to achieve a slimmer, more defined cheek contour. Their disclosures have helped normalize the procedure and illustrate that it can be performed safely in an outpatient setting under local anesthesia with intra‑oral incisions, leaving no external scars.
Potential Complications: While buccal fat removal is generally well‑tolerated, complications can arise. Reported issues include asymmetry, over‑reduction that creates an unnaturally hollow appearance, infection, hematoma, temporary numbness, and rare facial nerve injury. Proper patient selection—healthy adults with stable weight and no naturally narrow facial structure—combined with a board‑certified facial plastic surgeon skilled in precise intra‑oral dissection, minimizes these risks. Post‑operative care such as a soft diet, oral hygiene, and monitoring for signs of infection further supports optimal outcomes.
Patient Gallery and Long‑Term Satisfaction
 Our patient gallery displays before‑and‑after photos that illustrate a modest narrowing of the cheeks and a more defined jawline while preserving natural harmony. Ten‑year follow‑up data show most individuals keep a youthful, sculpted mid‑face; occasional age‑related volume loss can be corrected with fillers. Testimonials highlight confidence and lasting satisfaction and continued positive feedback from our team.
Conclusion – A Balanced, Personalized Approach to Mid‑Face Sculpting
Key Takeaways: Buccal fat removal thins the mid‑face by excising buccal fat pads through an intra‑oral incision, leaving no external scar. Results are permanent because the fat cells do not regenerate, although aging and weight changes can alter contour. Ideal candidates are healthy adults with full cheeks and expectations; thin‑boned or older patients may be unsuitable.
Importance of Expert Guidance: A board‑certified facial plastic surgeon must evaluate facial anatomy, skin elasticity, and skeletal proportions before deciding how much fat to remove. Precise technique protects the facial nerve, salivary ducts, and Stenson’s duct, reducing risks of asymmetry, infection, or numbness. Counseling sets goals and care.
Future Aesthetic Planning: Since buccal fat does not regrow, patients should anticipate loss and consider fillers, chin augmentation, or a mid‑face lift to preserve balance. Ongoing monitoring and a maintenance plan help maintain appearance.





Locations


© 2014 - 2025. Thomas W. Loeb | Board Certified Plastic Surgeon