.png)


.svg)
.svg)

Innovative Hybrid Strategies Elevate Nasolabial Fold Rejuvenation
News
/
April 14, 2026
Hybrid Approaches to Nasolabial Fold Correction: Combining Fillers and Surgery
Innovative Hybrid Strategies Elevate Nasolabial Fold Rejuvenation

Body contouring has revolutionized the way we think about self-care and aesthetic transformations. It’s more than just a cosmetic procedure—it’s a path to enhanced confidence and self-expression.
Why Nasolabial Folds Matter and the Rise of Hybrid Solutions
Nasolabial folds (NLFs), or smile lines, are an anatomical transition between the cheek and the nasojugal area. Their prominence increases with age because loss of collagen and elastin, flattening of the cheekbones, and gravitational descent cause volume depletion and ligament laxity. Environmental factors—sun exposure, smoking, and rapid weight change—exacerbate this process.
Treating NLFs with fillers alone restores superficial volume but cannot correct deep fibrous tethering or skeletal descent, often requiring repeat injections every 6‑12 months. Surgical lifts address deep tissue sagging and ligament release, yet they leave residual surface volume deficits and involve longer recovery.
A hybrid approach merges the immediate volumizing effect of hyaluronic‑acid or calcium‑hydroxylapatite fillers with minimally invasive surgical techniques such as limited SMAS tightening, sub‑cision, or thread lifts. This combination provides instant contour improvement, stimulates collagen remodeling, and supplies durable structural support, resulting in more natural, long‑lasting outcomes while reducing the amount of filler needed and the extent of surgical dissection.
Understanding Nasolabial Folds and First Treatment Landscape
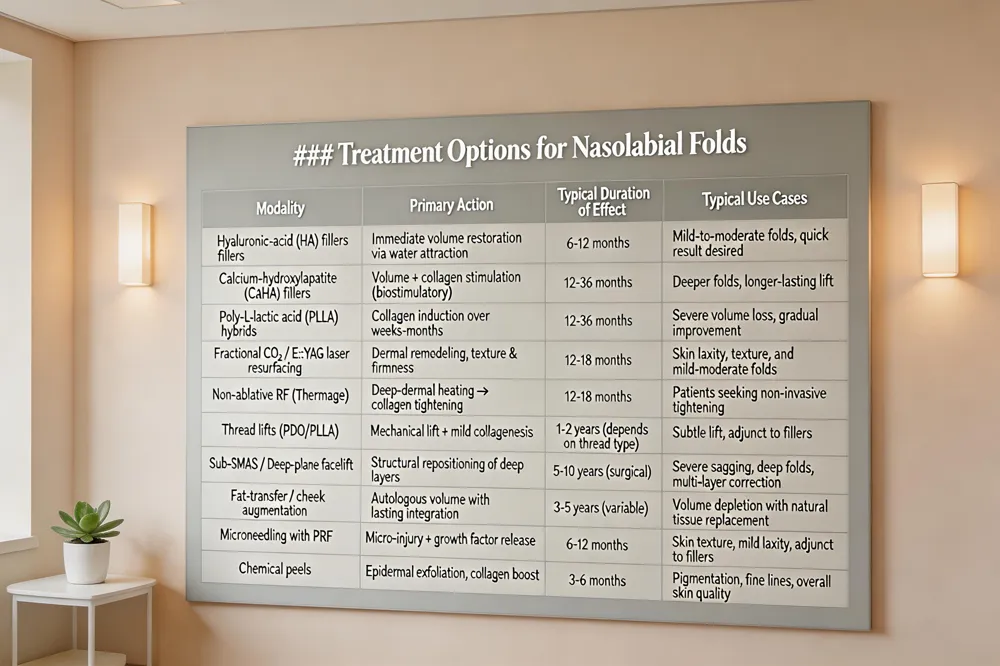 Nasolabial folds (NLFs) deepen primarily from age‑related loss of collagen, elastin, and sub‑cutaneous fat, combined with bone resorption, ligament laxity, sun damage, smoking and abrupt weight changes. Non‑surgical options include hyaluronic‑acid (HA) fillers, calcium‑hydroxylapatite (CaHA) or poly‑L‑lactic acid (PLLA) hybrids, laser or radio‑frequency resurfacing, microneedling, and thread lifts. HA fillers give immediate volume and last 6‑12 months; hybrid fillers add collagen stimulation and can extend results to 12‑36 months; laser and RF improve skin texture and firmness for 12‑18 months. Surgical lifts—sub‑SMAS, deep‑plane, or limited mid‑face lifts—reposition deep facial layers, correct ligamentous descent, and provide durable structural support that fillers alone cannot achieve.
Can nasolabial folds be corrected? Yes. Mild‑to‑moderate folds respond well to HA fillers, laser resurfacing, RF tightening, or thread lifts. Deep folds with significant sagging benefit from a surgical facelift, often combined with fat‑transfer or cheek augmentation for lasting, comprehensive improvement.
What are the top 5 aesthetic procedures? 1) Neurotoxin injections (Botox®) (Botox®, Dysport®, Xeomin®) for dynamic wrinkles; 2) HA dermal fillers (Restylane®, Juvéderm®, Voluma®) for volume restoration; 3) Microneedling with PRF to stimulate collagen; 4) Chemical peels for skin resurfacing; 5) Laser resurfacing to reduce fine lines, pigmentation, and texture issues.
What is the best skin tightening procedure for over 60? Fractional CO₂ or Er:YAG laser resurfacing offers deep collagen remodeling and lifts sagging tissue. When minimal downtime is required, non‑ablative radio‑frequency (Thermage) or micro‑focused ultrasound (Ultherapy) provide effective deep‑dermal tightening without aggressive surface removal.
Hybrid Filler Science: From HA to Advanced Biostimulatory Blends
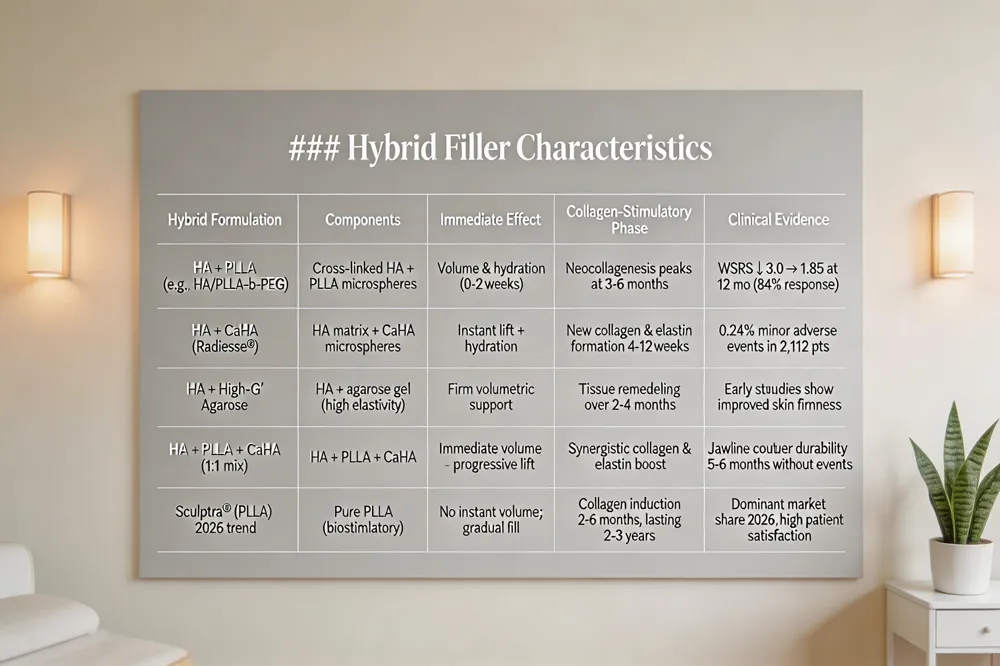 Hybrid dermal fillers combine cross‑linked hyaluronic acid (HA) with a biostimulatory component such as poly‑L‑lactic acid (PLLA), calcium‑hydroxylapatite (CaHA) microspheres, or high‑G′ agarose gel. HA supplies immediate hydration and volume by attracting water, while PLLA, CaHA, and agarose trigger neocollagenesis, elastin remodeling, and tissue tightening over weeks to months. Clinical data support this dual action: a retrospective analysis of 13 females treated with HA/PLLA‑b‑PEG showed WSRS scores drop from 3.0 to 1.85 at 12 months (84% response) and high FACE‑Q satisfaction. Larger series (2,112 patients) using a premixed CaHA:CPM‑HA blend reported only 0.24% minor adverse events, confirming safety.
Hybrid filler Radiesse: The hybrid Radiesse formulation mixes CaHA microspheres with a cohesive HA matrix, delivering instant lift and sustained collagen induction; Dr. Loeb uses it to refine jawline, cheekbones, and nasolabial folds for natural, progressive improvement.
What is the new filler in 2026? Sculptra Aesthetic, a biostimulatory PLLA filler, dominates 2026 trends, gradually restoring volume to cheeks, temples, and jawline through endogenous collagen production.
Jawline sharp contouring with hybrid filler: A 126‑patient series employed a 1:1 HA‑CPM‑CaHA mix via retrograde fanning (≈5.8 mL per mouth), achieving sharply defined jawlines that remained durable for months without adverse events.
Safety, Removal, and Cost Considerations in Hybrid Rejuvenation
 Hybrid facial rejuvenation blends dermal fillers with limited surgical adjuncts, demanding careful planning for safety, filler management, and budgeting.
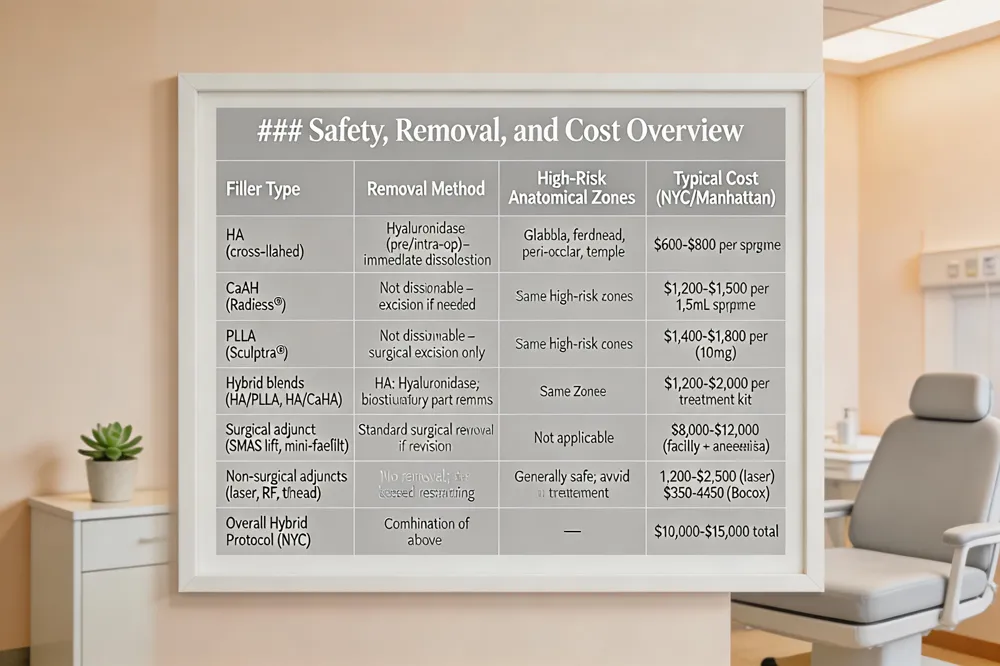
Management of fillers during surgery – Hyaluronic‑acid (HA) fillers can be dissolved with hyaluronidase before or intra‑operatively, allowing the gel to be resorbed and preventing interference with suturing. In procedures such as rhinoplasty or mid‑face lifts, the HA solution often exits as a clear fluid after needle aspiration. Biostimulatory agents (CaHA, PLLA) are not readily dissolvable; they are either left in place to integrate or excised in a controlled manner, acknowledging a small risk of scar tissue.
High‑risk filler locations and vascular safety – The glabella, forehead, peri‑ocular, and temple areas house dense arterial networks; inadvertent injection of high‑viscosity products (CaHA, PLLA) here carries the greatest risk of occlusion and visual loss. HA fillers, while more easily reversed, still demand blunt‑cannula technique and aspiration to avoid intravascular placement.
Financial aspects of combined treatments – Non‑surgical interventions typically cost $600‑$800 per HA syringe, $1,200‑$2,500 for laser resurfacing, and $350‑$450 for Botox. Surgical components such as a limited SMAS lift or sub‑mental fat graft add $8,000‑$12,000, plus anesthesia and facility fees. In Manhattan, prices often sit at the upper end of national ranges, making a hybrid protocol roughly $10,000‑$15,000 overall, depending on the number of filler sessions and surgical complexity.
Key take‑aways – Fillers can be removed or neutralized during surgery when using HA with hyaluronidase; permanent biostimulatory agents require meticulous handling. Vascular safety is paramount in high‑risk zones, especially with high‑viscosity fillers. Patients should be counseled on the cumulative cost of hybrid rejuvenation, which blends immediate non‑surgical benefits with the durable structural changes of surgery.
Hybrid Surgical Techniques that Amplify Filler Results
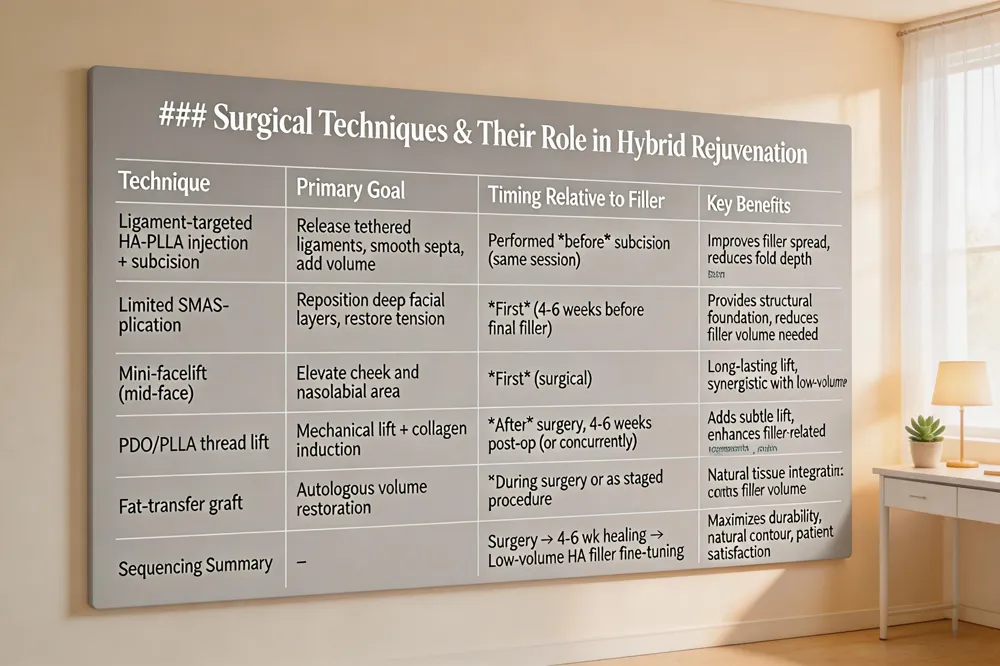 Ligament‑targeted injection and subcision Modern protocols begin with a ligament‑targeted filler placement that releases the temporal, preauricular, zygomatic and mandibular retaining ligaments. A blunt‑tip micro‑cannula delivers a HA‑PLLA‑b‑PEG hybrid filler (or HA‑CaHA blend) into the deep‑dermal plane, providing immediate volume while the PLLA component stimulates collagen for up to 12 months. Subcision of fibrous septa follows, loosening tethered tissue and priming the fold for smoother filler distribution.
Limited SMAS‑plication, thread lifts, and mini‑facelifts For patients with moderate‑to‑severe folds, a Limited SMAS‑plication or mini‑facelift repositions deep facial layers, restores ligament tension, and reduces gravity‑related descent. Absorbable PDO or PLLA threads can be added to achieve a subtle lift and further collagen remodeling. These minimally invasive adjuncts complement the volumetric gain of fillers and reduce the need for large filler volumes.
Sequencing of surgery and filler for optimal outcome The preferred sequence is surgery first (SMAS‑plication or thread lift), allowing tissue to heal for 4‑6 weeks, followed by low‑volume HA‑based filler to fine‑tune contour and hydrate the skin. This staged approach yields a natural, durable result with higher patient satisfaction.
Best treatment for nasolabial folds A hyaluronic‑acid filler (Juvederm®/Restylane®) offers instant volume for 6‑12 months; for deeper folds Dr. Loeb adds collagen‑stimulating CaHA or PLLA fillers and may incorporate a subtle sub‑muscular fat graft or thread lift for lasting structural support.
How do celebrities get rid of nasolabial folds? Celebrities typically start with HA fillers for rapid smoothing, layer Radiesse or PLLA for longer‑lasting lift, use smooth thread procedures for a non‑surgical elevation, and resort to facelift or direct nasolabial‑fold excision when folds are profound.
Cosmetic procedures list Dr. Thomas W. Loeb offers facelifts, brow lifts, blepharoplasty, rhinoplasty, chin/jawline contouring, otoplasty, neurotoxin injections, dermal fillers (HA, CaHA, PLLA), chemical peels, laser resurfacing, microneedling, skin‑rejuvenation protocols, liposuction, abdominoplasty, brachioplasty, buttock augmentation, laser hair removal, scar revision, and personalized skincare regimens.
Personalized Hybrid Planning at Dr. Loeb’s Boutique Practice
 A successful nasolabial‑fold rejuvenation begins with a comprehensive facial analysis that evaluates skin quality, bone structure, ligamentous support, and the patient’s aesthetic goals. Dr. Thomas Loeb’s practice uses 3‑D imaging and a detailed assessment of wrinkle severity (WSRS), volume loss, and soft‑tissue laxity to design a customized hybrid plan. The protocol tailors the ratio of hyaluronic‑acid (HA) to biostimulatory filler (e.g., poly‑L‑lactic acid or calcium‑hydroxyapatite and selects injection planes—superficial dermal for fine lines, deep‑dermal or supraperiosteal for structural lift—while coordinating surgical vectors such as limited SMAS‑plication or mid‑face lift. This layered approach delivers immediate volumization from HA and long‑term collagen stimulation from the biostimulatory component, with surgery providing durable tissue repositioning. Post‑treatment care includes sun protection (SPF 30+), smoking cessation, gentle skin hygiene, and a brief cooling‑off period before any additional filler touch‑ups. Maintenance visits are scheduled at 6‑ and 12‑month intervals to assess WSRS scores, GAIS improvement, and patient‑reported satisfaction, allowing timely adjustments and ensuring lasting, natural‑looking results.
Achieving Natural, Long‑Lasting Harmony with Hybrid Rejuvenation
Hybrid rejuvenation for nasolabial folds leverages the instant volumizing power of hyaluronic‑acid (HA) fillers while a durable surgical lift restores deep tissue tension and structural support. By injecting HA (or HA‑based hybrids) into the superficial planes, clinicians achieve immediate contour smoothing; a subsequent limited SMAS or sub‑SMAS lift repositions retaining ligaments and cheek fat, extending the aesthetic result beyond the typical 6‑12 month filler lifespan. This synergy minimizes the volume of filler required, reduces over‑correction risk, and yields a natural, gradual transition from lift to filler‑enhanced contour.
Safety is paramount: blunt‑cannula techniques, aspiration, and staged timing (often 2‑4 weeks pre‑ or post‑surgery) lower complications such as vascular occlusion, nodules, or infection. Experienced surgeons blend artistry with anatomy, tailoring injection depth, filler type (HA, CaHA, PLLA, or agar‑HA hybrids) and surgical vectors to each patient’s facial architecture and aesthetic goals.
Long‑term success depends on ongoing care—sun protection, smoking cessation, and a skin‑care regimen that supports collagen production. Regular follow‑up visits allow fine‑tuning with touch‑up fillers and monitoring of surgical healing, ensuring sustained patient satisfaction and harmonious facial rejuvenation.
Why Nasolabial Folds Matter and the Rise of Hybrid Solutions
Nasolabial folds (NLFs), or smile lines, are an anatomical transition between the cheek and the nasojugal area. Their prominence increases with age because loss of collagen and elastin, flattening of the cheekbones, and gravitational descent cause volume depletion and ligament laxity. Environmental factors—sun exposure, smoking, and rapid weight change—exacerbate this process.
Treating NLFs with fillers alone restores superficial volume but cannot correct deep fibrous tethering or skeletal descent, often requiring repeat injections every 6‑12 months. Surgical lifts address deep tissue sagging and ligament release, yet they leave residual surface volume deficits and involve longer recovery.
A hybrid approach merges the immediate volumizing effect of hyaluronic‑acid or calcium‑hydroxylapatite fillers with minimally invasive surgical techniques such as limited SMAS tightening, sub‑cision, or thread lifts. This combination provides instant contour improvement, stimulates collagen remodeling, and supplies durable structural support, resulting in more natural, long‑lasting outcomes while reducing the amount of filler needed and the extent of surgical dissection.
Understanding Nasolabial Folds and First Treatment Landscape
 Nasolabial folds (NLFs) deepen primarily from age‑related loss of collagen, elastin, and sub‑cutaneous fat, combined with bone resorption, ligament laxity, sun damage, smoking and abrupt weight changes. Non‑surgical options include hyaluronic‑acid (HA) fillers, calcium‑hydroxylapatite (CaHA) or poly‑L‑lactic acid (PLLA) hybrids, laser or radio‑frequency resurfacing, microneedling, and thread lifts. HA fillers give immediate volume and last 6‑12 months; hybrid fillers add collagen stimulation and can extend results to 12‑36 months; laser and RF improve skin texture and firmness for 12‑18 months. Surgical lifts—sub‑SMAS, deep‑plane, or limited mid‑face lifts—reposition deep facial layers, correct ligamentous descent, and provide durable structural support that fillers alone cannot achieve.
Can nasolabial folds be corrected? Yes. Mild‑to‑moderate folds respond well to HA fillers, laser resurfacing, RF tightening, or thread lifts. Deep folds with significant sagging benefit from a surgical facelift, often combined with fat‑transfer or cheek augmentation for lasting, comprehensive improvement.
What are the top 5 aesthetic procedures? 1) Neurotoxin injections (Botox®) (Botox®, Dysport®, Xeomin®) for dynamic wrinkles; 2) HA dermal fillers (Restylane®, Juvéderm®, Voluma®) for volume restoration; 3) Microneedling with PRF to stimulate collagen; 4) Chemical peels for skin resurfacing; 5) Laser resurfacing to reduce fine lines, pigmentation, and texture issues.
What is the best skin tightening procedure for over 60? Fractional CO₂ or Er:YAG laser resurfacing offers deep collagen remodeling and lifts sagging tissue. When minimal downtime is required, non‑ablative radio‑frequency (Thermage) or micro‑focused ultrasound (Ultherapy) provide effective deep‑dermal tightening without aggressive surface removal.
Hybrid Filler Science: From HA to Advanced Biostimulatory Blends
 Hybrid dermal fillers combine cross‑linked hyaluronic acid (HA) with a biostimulatory component such as poly‑L‑lactic acid (PLLA), calcium‑hydroxylapatite (CaHA) microspheres, or high‑G′ agarose gel. HA supplies immediate hydration and volume by attracting water, while PLLA, CaHA, and agarose trigger neocollagenesis, elastin remodeling, and tissue tightening over weeks to months. Clinical data support this dual action: a retrospective analysis of 13 females treated with HA/PLLA‑b‑PEG showed WSRS scores drop from 3.0 to 1.85 at 12 months (84% response) and high FACE‑Q satisfaction. Larger series (2,112 patients) using a premixed CaHA:CPM‑HA blend reported only 0.24% minor adverse events, confirming safety.
Hybrid filler Radiesse: The hybrid Radiesse formulation mixes CaHA microspheres with a cohesive HA matrix, delivering instant lift and sustained collagen induction; Dr. Loeb uses it to refine jawline, cheekbones, and nasolabial folds for natural, progressive improvement.
What is the new filler in 2026? Sculptra Aesthetic, a biostimulatory PLLA filler, dominates 2026 trends, gradually restoring volume to cheeks, temples, and jawline through endogenous collagen production.
Jawline sharp contouring with hybrid filler: A 126‑patient series employed a 1:1 HA‑CPM‑CaHA mix via retrograde fanning (≈5.8 mL per mouth), achieving sharply defined jawlines that remained durable for months without adverse events.
Safety, Removal, and Cost Considerations in Hybrid Rejuvenation
 Hybrid facial rejuvenation blends dermal fillers with limited surgical adjuncts, demanding careful planning for safety, filler management, and budgeting.
Management of fillers during surgery – Hyaluronic‑acid (HA) fillers can be dissolved with hyaluronidase before or intra‑operatively, allowing the gel to be resorbed and preventing interference with suturing. In procedures such as rhinoplasty or mid‑face lifts, the HA solution often exits as a clear fluid after needle aspiration. Biostimulatory agents (CaHA, PLLA) are not readily dissolvable; they are either left in place to integrate or excised in a controlled manner, acknowledging a small risk of scar tissue.
High‑risk filler locations and vascular safety – The glabella, forehead, peri‑ocular, and temple areas house dense arterial networks; inadvertent injection of high‑viscosity products (CaHA, PLLA) here carries the greatest risk of occlusion and visual loss. HA fillers, while more easily reversed, still demand blunt‑cannula technique and aspiration to avoid intravascular placement.
Financial aspects of combined treatments – Non‑surgical interventions typically cost $600‑$800 per HA syringe, $1,200‑$2,500 for laser resurfacing, and $350‑$450 for Botox. Surgical components such as a limited SMAS lift or sub‑mental fat graft add $8,000‑$12,000, plus anesthesia and facility fees. In Manhattan, prices often sit at the upper end of national ranges, making a hybrid protocol roughly $10,000‑$15,000 overall, depending on the number of filler sessions and surgical complexity.
Key take‑aways – Fillers can be removed or neutralized during surgery when using HA with hyaluronidase; permanent biostimulatory agents require meticulous handling. Vascular safety is paramount in high‑risk zones, especially with high‑viscosity fillers. Patients should be counseled on the cumulative cost of hybrid rejuvenation, which blends immediate non‑surgical benefits with the durable structural changes of surgery.
Hybrid Surgical Techniques that Amplify Filler Results
 Ligament‑targeted injection and subcision Modern protocols begin with a ligament‑targeted filler placement that releases the temporal, preauricular, zygomatic and mandibular retaining ligaments. A blunt‑tip micro‑cannula delivers a HA‑PLLA‑b‑PEG hybrid filler (or HA‑CaHA blend) into the deep‑dermal plane, providing immediate volume while the PLLA component stimulates collagen for up to 12 months. Subcision of fibrous septa follows, loosening tethered tissue and priming the fold for smoother filler distribution.
Limited SMAS‑plication, thread lifts, and mini‑facelifts For patients with moderate‑to‑severe folds, a Limited SMAS‑plication or mini‑facelift repositions deep facial layers, restores ligament tension, and reduces gravity‑related descent. Absorbable PDO or PLLA threads can be added to achieve a subtle lift and further collagen remodeling. These minimally invasive adjuncts complement the volumetric gain of fillers and reduce the need for large filler volumes.
Sequencing of surgery and filler for optimal outcome The preferred sequence is surgery first (SMAS‑plication or thread lift), allowing tissue to heal for 4‑6 weeks, followed by low‑volume HA‑based filler to fine‑tune contour and hydrate the skin. This staged approach yields a natural, durable result with higher patient satisfaction.
Best treatment for nasolabial folds A hyaluronic‑acid filler (Juvederm®/Restylane®) offers instant volume for 6‑12 months; for deeper folds Dr. Loeb adds collagen‑stimulating CaHA or PLLA fillers and may incorporate a subtle sub‑muscular fat graft or thread lift for lasting structural support.
How do celebrities get rid of nasolabial folds? Celebrities typically start with HA fillers for rapid smoothing, layer Radiesse or PLLA for longer‑lasting lift, use smooth thread procedures for a non‑surgical elevation, and resort to facelift or direct nasolabial‑fold excision when folds are profound.
Cosmetic procedures list Dr. Thomas W. Loeb offers facelifts, brow lifts, blepharoplasty, rhinoplasty, chin/jawline contouring, otoplasty, neurotoxin injections, dermal fillers (HA, CaHA, PLLA), chemical peels, laser resurfacing, microneedling, skin‑rejuvenation protocols, liposuction, abdominoplasty, brachioplasty, buttock augmentation, laser hair removal, scar revision, and personalized skincare regimens.
Personalized Hybrid Planning at Dr. Loeb’s Boutique Practice
 A successful nasolabial‑fold rejuvenation begins with a comprehensive facial analysis that evaluates skin quality, bone structure, ligamentous support, and the patient’s aesthetic goals. Dr. Thomas Loeb’s practice uses 3‑D imaging and a detailed assessment of wrinkle severity (WSRS), volume loss, and soft‑tissue laxity to design a customized hybrid plan. The protocol tailors the ratio of hyaluronic‑acid (HA) to biostimulatory filler (e.g., poly‑L‑lactic acid or calcium‑hydroxyapatite and selects injection planes—superficial dermal for fine lines, deep‑dermal or supraperiosteal for structural lift—while coordinating surgical vectors such as limited SMAS‑plication or mid‑face lift. This layered approach delivers immediate volumization from HA and long‑term collagen stimulation from the biostimulatory component, with surgery providing durable tissue repositioning. Post‑treatment care includes sun protection (SPF 30+), smoking cessation, gentle skin hygiene, and a brief cooling‑off period before any additional filler touch‑ups. Maintenance visits are scheduled at 6‑ and 12‑month intervals to assess WSRS scores, GAIS improvement, and patient‑reported satisfaction, allowing timely adjustments and ensuring lasting, natural‑looking results.
Achieving Natural, Long‑Lasting Harmony with Hybrid Rejuvenation
Hybrid rejuvenation for nasolabial folds leverages the instant volumizing power of hyaluronic‑acid (HA) fillers while a durable surgical lift restores deep tissue tension and structural support. By injecting HA (or HA‑based hybrids) into the superficial planes, clinicians achieve immediate contour smoothing; a subsequent limited SMAS or sub‑SMAS lift repositions retaining ligaments and cheek fat, extending the aesthetic result beyond the typical 6‑12 month filler lifespan. This synergy minimizes the volume of filler required, reduces over‑correction risk, and yields a natural, gradual transition from lift to filler‑enhanced contour.
Safety is paramount: blunt‑cannula techniques, aspiration, and staged timing (often 2‑4 weeks pre‑ or post‑surgery) lower complications such as vascular occlusion, nodules, or infection. Experienced surgeons blend artistry with anatomy, tailoring injection depth, filler type (HA, CaHA, PLLA, or agar‑HA hybrids) and surgical vectors to each patient’s facial architecture and aesthetic goals.
Long‑term success depends on ongoing care—sun protection, smoking cessation, and a skin‑care regimen that supports collagen production. Regular follow‑up visits allow fine‑tuning with touch‑up fillers and monitoring of surgical healing, ensuring sustained patient satisfaction and harmonious facial rejuvenation.
Heading
Why Nasolabial Folds Matter and the Rise of Hybrid Solutions
Nasolabial folds (NLFs), or smile lines, are an anatomical transition between the cheek and the nasojugal area. Their prominence increases with age because loss of collagen and elastin, flattening of the cheekbones, and gravitational descent cause volume depletion and ligament laxity. Environmental factors—sun exposure, smoking, and rapid weight change—exacerbate this process.
Treating NLFs with fillers alone restores superficial volume but cannot correct deep fibrous tethering or skeletal descent, often requiring repeat injections every 6‑12 months. Surgical lifts address deep tissue sagging and ligament release, yet they leave residual surface volume deficits and involve longer recovery.
A hybrid approach merges the immediate volumizing effect of hyaluronic‑acid or calcium‑hydroxylapatite fillers with minimally invasive surgical techniques such as limited SMAS tightening, sub‑cision, or thread lifts. This combination provides instant contour improvement, stimulates collagen remodeling, and supplies durable structural support, resulting in more natural, long‑lasting outcomes while reducing the amount of filler needed and the extent of surgical dissection.
Understanding Nasolabial Folds and First Treatment Landscape
 Nasolabial folds (NLFs) deepen primarily from age‑related loss of collagen, elastin, and sub‑cutaneous fat, combined with bone resorption, ligament laxity, sun damage, smoking and abrupt weight changes. Non‑surgical options include hyaluronic‑acid (HA) fillers, calcium‑hydroxylapatite (CaHA) or poly‑L‑lactic acid (PLLA) hybrids, laser or radio‑frequency resurfacing, microneedling, and thread lifts. HA fillers give immediate volume and last 6‑12 months; hybrid fillers add collagen stimulation and can extend results to 12‑36 months; laser and RF improve skin texture and firmness for 12‑18 months. Surgical lifts—sub‑SMAS, deep‑plane, or limited mid‑face lifts—reposition deep facial layers, correct ligamentous descent, and provide durable structural support that fillers alone cannot achieve.
Can nasolabial folds be corrected? Yes. Mild‑to‑moderate folds respond well to HA fillers, laser resurfacing, RF tightening, or thread lifts. Deep folds with significant sagging benefit from a surgical facelift, often combined with fat‑transfer or cheek augmentation for lasting, comprehensive improvement.
What are the top 5 aesthetic procedures? 1) Neurotoxin injections (Botox®) (Botox®, Dysport®, Xeomin®) for dynamic wrinkles; 2) HA dermal fillers (Restylane®, Juvéderm®, Voluma®) for volume restoration; 3) Microneedling with PRF to stimulate collagen; 4) Chemical peels for skin resurfacing; 5) Laser resurfacing to reduce fine lines, pigmentation, and texture issues.
What is the best skin tightening procedure for over 60? Fractional CO₂ or Er:YAG laser resurfacing offers deep collagen remodeling and lifts sagging tissue. When minimal downtime is required, non‑ablative radio‑frequency (Thermage) or micro‑focused ultrasound (Ultherapy) provide effective deep‑dermal tightening without aggressive surface removal.
Hybrid Filler Science: From HA to Advanced Biostimulatory Blends
 Hybrid dermal fillers combine cross‑linked hyaluronic acid (HA) with a biostimulatory component such as poly‑L‑lactic acid (PLLA), calcium‑hydroxylapatite (CaHA) microspheres, or high‑G′ agarose gel. HA supplies immediate hydration and volume by attracting water, while PLLA, CaHA, and agarose trigger neocollagenesis, elastin remodeling, and tissue tightening over weeks to months. Clinical data support this dual action: a retrospective analysis of 13 females treated with HA/PLLA‑b‑PEG showed WSRS scores drop from 3.0 to 1.85 at 12 months (84% response) and high FACE‑Q satisfaction. Larger series (2,112 patients) using a premixed CaHA:CPM‑HA blend reported only 0.24% minor adverse events, confirming safety.
Hybrid filler Radiesse: The hybrid Radiesse formulation mixes CaHA microspheres with a cohesive HA matrix, delivering instant lift and sustained collagen induction; Dr. Loeb uses it to refine jawline, cheekbones, and nasolabial folds for natural, progressive improvement.
What is the new filler in 2026? Sculptra Aesthetic, a biostimulatory PLLA filler, dominates 2026 trends, gradually restoring volume to cheeks, temples, and jawline through endogenous collagen production.
Jawline sharp contouring with hybrid filler: A 126‑patient series employed a 1:1 HA‑CPM‑CaHA mix via retrograde fanning (≈5.8 mL per mouth), achieving sharply defined jawlines that remained durable for months without adverse events.
Safety, Removal, and Cost Considerations in Hybrid Rejuvenation
 Hybrid facial rejuvenation blends dermal fillers with limited surgical adjuncts, demanding careful planning for safety, filler management, and budgeting.
Management of fillers during surgery – Hyaluronic‑acid (HA) fillers can be dissolved with hyaluronidase before or intra‑operatively, allowing the gel to be resorbed and preventing interference with suturing. In procedures such as rhinoplasty or mid‑face lifts, the HA solution often exits as a clear fluid after needle aspiration. Biostimulatory agents (CaHA, PLLA) are not readily dissolvable; they are either left in place to integrate or excised in a controlled manner, acknowledging a small risk of scar tissue.
High‑risk filler locations and vascular safety – The glabella, forehead, peri‑ocular, and temple areas house dense arterial networks; inadvertent injection of high‑viscosity products (CaHA, PLLA) here carries the greatest risk of occlusion and visual loss. HA fillers, while more easily reversed, still demand blunt‑cannula technique and aspiration to avoid intravascular placement.
Financial aspects of combined treatments – Non‑surgical interventions typically cost $600‑$800 per HA syringe, $1,200‑$2,500 for laser resurfacing, and $350‑$450 for Botox. Surgical components such as a limited SMAS lift or sub‑mental fat graft add $8,000‑$12,000, plus anesthesia and facility fees. In Manhattan, prices often sit at the upper end of national ranges, making a hybrid protocol roughly $10,000‑$15,000 overall, depending on the number of filler sessions and surgical complexity.
Key take‑aways – Fillers can be removed or neutralized during surgery when using HA with hyaluronidase; permanent biostimulatory agents require meticulous handling. Vascular safety is paramount in high‑risk zones, especially with high‑viscosity fillers. Patients should be counseled on the cumulative cost of hybrid rejuvenation, which blends immediate non‑surgical benefits with the durable structural changes of surgery.
Hybrid Surgical Techniques that Amplify Filler Results
 Ligament‑targeted injection and subcision Modern protocols begin with a ligament‑targeted filler placement that releases the temporal, preauricular, zygomatic and mandibular retaining ligaments. A blunt‑tip micro‑cannula delivers a HA‑PLLA‑b‑PEG hybrid filler (or HA‑CaHA blend) into the deep‑dermal plane, providing immediate volume while the PLLA component stimulates collagen for up to 12 months. Subcision of fibrous septa follows, loosening tethered tissue and priming the fold for smoother filler distribution.
Limited SMAS‑plication, thread lifts, and mini‑facelifts For patients with moderate‑to‑severe folds, a Limited SMAS‑plication or mini‑facelift repositions deep facial layers, restores ligament tension, and reduces gravity‑related descent. Absorbable PDO or PLLA threads can be added to achieve a subtle lift and further collagen remodeling. These minimally invasive adjuncts complement the volumetric gain of fillers and reduce the need for large filler volumes.
Sequencing of surgery and filler for optimal outcome The preferred sequence is surgery first (SMAS‑plication or thread lift), allowing tissue to heal for 4‑6 weeks, followed by low‑volume HA‑based filler to fine‑tune contour and hydrate the skin. This staged approach yields a natural, durable result with higher patient satisfaction.
Best treatment for nasolabial folds A hyaluronic‑acid filler (Juvederm®/Restylane®) offers instant volume for 6‑12 months; for deeper folds Dr. Loeb adds collagen‑stimulating CaHA or PLLA fillers and may incorporate a subtle sub‑muscular fat graft or thread lift for lasting structural support.
How do celebrities get rid of nasolabial folds? Celebrities typically start with HA fillers for rapid smoothing, layer Radiesse or PLLA for longer‑lasting lift, use smooth thread procedures for a non‑surgical elevation, and resort to facelift or direct nasolabial‑fold excision when folds are profound.
Cosmetic procedures list Dr. Thomas W. Loeb offers facelifts, brow lifts, blepharoplasty, rhinoplasty, chin/jawline contouring, otoplasty, neurotoxin injections, dermal fillers (HA, CaHA, PLLA), chemical peels, laser resurfacing, microneedling, skin‑rejuvenation protocols, liposuction, abdominoplasty, brachioplasty, buttock augmentation, laser hair removal, scar revision, and personalized skincare regimens.
Personalized Hybrid Planning at Dr. Loeb’s Boutique Practice
 A successful nasolabial‑fold rejuvenation begins with a comprehensive facial analysis that evaluates skin quality, bone structure, ligamentous support, and the patient’s aesthetic goals. Dr. Thomas Loeb’s practice uses 3‑D imaging and a detailed assessment of wrinkle severity (WSRS), volume loss, and soft‑tissue laxity to design a customized hybrid plan. The protocol tailors the ratio of hyaluronic‑acid (HA) to biostimulatory filler (e.g., poly‑L‑lactic acid or calcium‑hydroxyapatite and selects injection planes—superficial dermal for fine lines, deep‑dermal or supraperiosteal for structural lift—while coordinating surgical vectors such as limited SMAS‑plication or mid‑face lift. This layered approach delivers immediate volumization from HA and long‑term collagen stimulation from the biostimulatory component, with surgery providing durable tissue repositioning. Post‑treatment care includes sun protection (SPF 30+), smoking cessation, gentle skin hygiene, and a brief cooling‑off period before any additional filler touch‑ups. Maintenance visits are scheduled at 6‑ and 12‑month intervals to assess WSRS scores, GAIS improvement, and patient‑reported satisfaction, allowing timely adjustments and ensuring lasting, natural‑looking results.
Achieving Natural, Long‑Lasting Harmony with Hybrid Rejuvenation
Hybrid rejuvenation for nasolabial folds leverages the instant volumizing power of hyaluronic‑acid (HA) fillers while a durable surgical lift restores deep tissue tension and structural support. By injecting HA (or HA‑based hybrids) into the superficial planes, clinicians achieve immediate contour smoothing; a subsequent limited SMAS or sub‑SMAS lift repositions retaining ligaments and cheek fat, extending the aesthetic result beyond the typical 6‑12 month filler lifespan. This synergy minimizes the volume of filler required, reduces over‑correction risk, and yields a natural, gradual transition from lift to filler‑enhanced contour.
Safety is paramount: blunt‑cannula techniques, aspiration, and staged timing (often 2‑4 weeks pre‑ or post‑surgery) lower complications such as vascular occlusion, nodules, or infection. Experienced surgeons blend artistry with anatomy, tailoring injection depth, filler type (HA, CaHA, PLLA, or agar‑HA hybrids) and surgical vectors to each patient’s facial architecture and aesthetic goals.
Long‑term success depends on ongoing care—sun protection, smoking cessation, and a skin‑care regimen that supports collagen production. Regular follow‑up visits allow fine‑tuning with touch‑up fillers and monitoring of surgical healing, ensuring sustained patient satisfaction and harmonious facial rejuvenation.





Locations


© 2014 - 2025. Thomas W. Loeb | Board Certified Plastic Surgeon