.png)


.svg)
.svg)

Achieving Natural Nipple and Areola Results: A Comprehensive Guide
News
/
April 16, 2026
Nipple and Areola Enhancement: Techniques for a Natural Look
Achieving Natural Nipple and Areola Results: A Comprehensive Guide

Body contouring has revolutionized the way we think about self-care and aesthetic transformations. It’s more than just a cosmetic procedure—it’s a path to enhanced confidence and self-expression.
Why Natural‑Looking Nipple & Areola Enhancement Matters
Patients seeking breast augmentation or reconstruction expect a result that looks and feels like their own tissue; the nipple‑areola complex (NAC) is the visual focal point that determines whether the breast appears natural or prosthetic. A proportionate areola (30–45 mm) with a subtle darker rim and a nipple projection of 4–8 mm creates harmonious balance and preserves the illusion of normal anatomy. Achieving this balance requires a tailored mix of surgical and non‑surgical options. Surgical techniques—such as periareolar excision for areola reduction, local flap reconstruction (C‑V, star, or donut flaps) for nipple projection, and autologous grafts—address size, shape, and texture while maintaining neurovascular integrity. Non‑surgical adjuncts, including 3‑D medical tattooing, hyaluronic‑acid fillers, and nipple prosthetics, fine‑tune color, shading, and temporary projection without additional incisions. Selecting the appropriate combination, guided by board‑certified surgeons, ensures realistic aesthetics, optimal healing, and lasting patient satisfaction.
Surgical Foundations: Flaps, Grafts, and Reduction Techniques
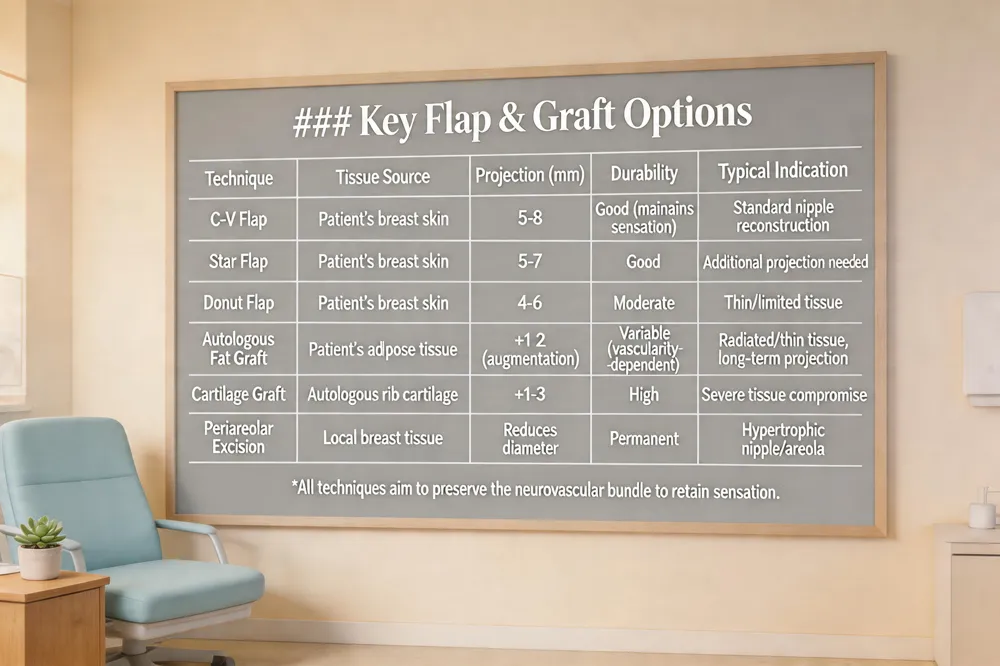 Local flap designs remain the cornerstone for achieving a natural‑looking nipple projection. The C‑V, star, skate, and donut flaps use the patient’s own breast skin, preserving the neurovascular bundle and tactile sensation while creating a three‑dimensional nipple. When tissue quality is compromised—such as after radiation or in very thin breasts—autologous grafts (fat, dermal matrix, or cartilage) can be incorporated into the flap core to augment volume and prolong projection.
For hypertrophic nipples or oversized areolas, periareolar excision, wedge resection, and circumferential reduction techniques remove excess skin and pigment while maintaining the pigmented rim for a seamless transition. These procedures are performed through a single, well‑placed incision that minimizes scarring and protects blood flow.
Preserving neurovascular supply is essential; surgeons avoid full‑thickness circumferential incisions and use meticulous suturing to maintain perfusion and sensation.
Answer to the question: Local skin flaps—particularly the C‑V, star, and donut designs—provide the most natural nipple projection because they use the patient’s native tissue and retain sensation. Adding autologous fat grafts or cartilage grafts can further enhance durability, especially in radiated or thin tissue.
Non‑Surgical Enhancements: Medical Tattooing, Fillers, and Prosthetics
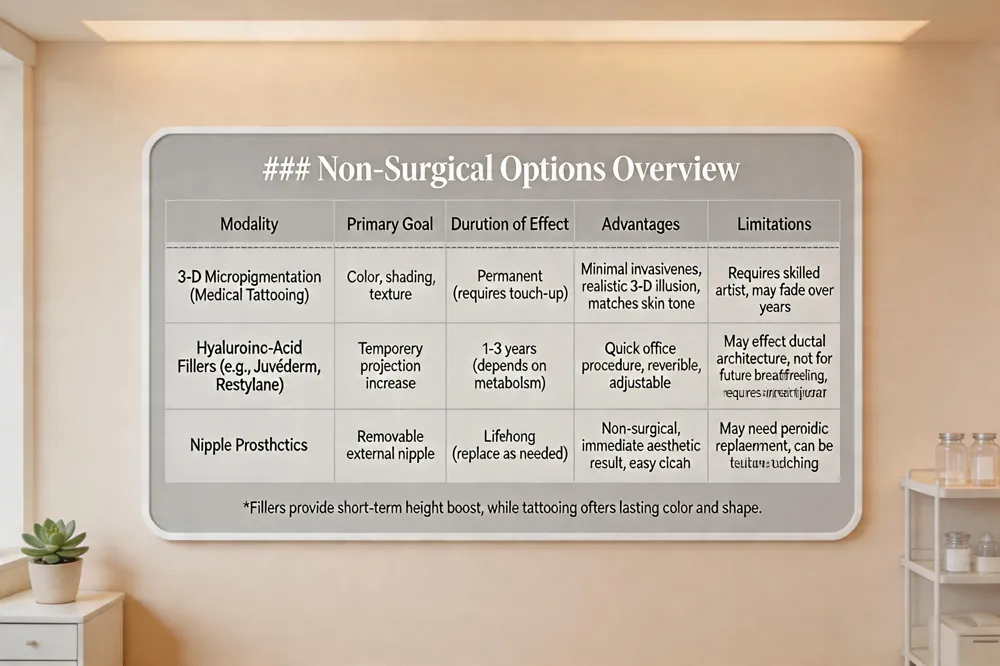 Medical‑grade 3‑D tattooing (micropigmentation) is now a standard, minimally invasive option for recreating the color, shading and texture of the nipple‑areola complex. Advanced 3‑D techniques blend a darker central nipple hue with a lighter peripheral rim, producing a realistic three‑dimensional illusion in a single session and offering a broad palette that matches the patient’s natural skin tone.
Hyaluronic‑acid fillers such as Juvéderm or Restylane can be injected beneath the nipple to add temporary projection. The procedure is performed with a fine needle in an office setting, usually requiring only one syringe per side and allowing patients to resume normal activities within 1–2 days. Projection gains last several years, but the filler does not provide permanent support and may disrupt ductal architecture, so surgeons advise deferring treatment until childbearing is complete and breastfeeding is no longer planned.
Nipple prosthetics provide a removable, non‑surgical alternative for patients who prefer not to undergo surgery or tattooing. Modern prosthetics mimic the look and feel of a natural nipple and can be fitted to the breast mound after reconstruction or augmentation.
Can injectable fillers replace surgery for nipple projection? Injectable hyaluronic‑acid fillers can increase nipple height for a few years with a quick, office‑based procedure, yet they are temporary, may affect ductal structures, and are generally not recommended for women planning future pregnancy or breastfeeding. Surgical options remain the definitive solution for lasting projection.
Timing, Eligibility, and Patient‑Specific Factors
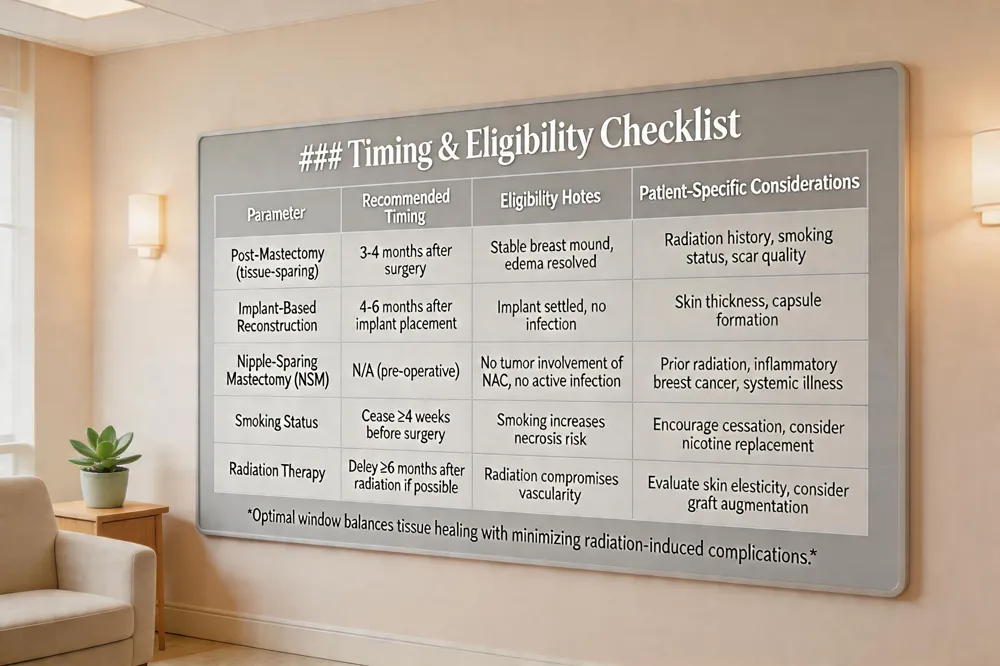 Nipple reconstruction is most successful when performed after the breast mound has stabilized. In practice, surgeons schedule the procedure 3–4 months after tissue‑sparing mastectomy or autologous flap reconstruction, allowing postoperative edema to resolve and incisional healing to mature. For implant‑based reconstruction, a slightly longer interval of 4–6 months is common to ensure the implant position is permanent before local flaps or grafts are created.
Eligibility for nipple‑sparing mastectomy (NSM) is limited by oncologic factors. Patients with inflammatory breast cancer, tumors involving the nipple‑areola complex, or cancer‑related nipple discharge are excluded because preserving the NAC could leave residual disease. Likewise, active infection or uncontrolled systemic illness contraindicates NSM.
Patient‑specific variables strongly influence outcomes. Prior radiation therapy compromises skin elasticity and vascularity, increasing the risk of nipple necrosis or loss of projection. Smoking diminishes microcirculation and impairs wound healing, while dense scar tissue or a thinned skin envelope can limit flap viability. Pre‑operative assessment should therefore include a detailed history of radiation, smoking status, and scar quality.
Modern planning tools mitigate these risks. High‑resolution 3‑D imaging and digital simulation allow the surgeon to visualize the final nipple‑areola complex, predict symmetry, and customize flap dimensions. Such personalized planning improves aesthetic predictability and helps set realistic patient expectations.
When is the optimal window for nipple reconstruction? Most surgeons schedule nipple reconstruction 3‑4 months after the breast mound is created, allowing swelling to subside and tissue to heal. For implant‑based reconstruction, a 4‑6 month interval is common to ensure stable positioning before flap or graft work.
Managing Risks, Recovery, and Long‑Term Aesthetic Refinement
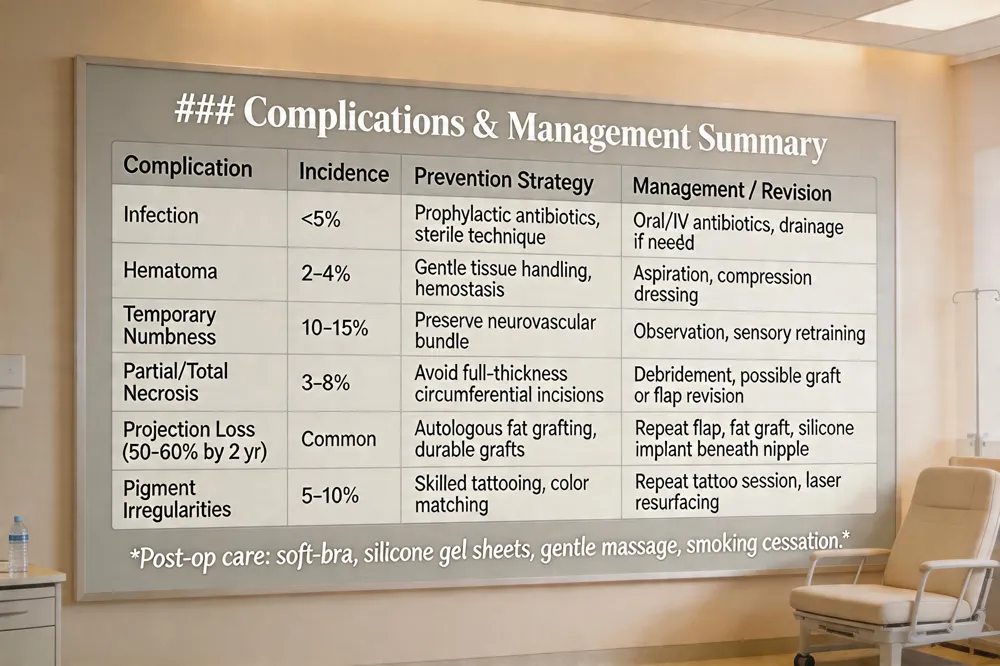 Nipple reconstruction, whether performed with local skin flaps, grafts, or medical tattooing, carries a low but meaningful complication profile. The most common issues include infection, hematoma, temporary numbness, partial or total necrosis of the reconstructed nipple, loss of projection (often 50‑60 % within two years), and pigment irregularities such as fading or uneven color match. Meticulous flap design that preserves neurovascular supply, gentle handling of tissue, and prophylactic antibiotics help mitigate these risks.
Post‑operative care is essential for optimal healing. Patients are instructed to keep the nipple‑areola complex protected from friction, wear a soft, non‑underwired bra after dressing removal, and apply silicone gel sheets to the scar to improve texture. Gentle massage of the surrounding breast tissue promotes circulation, while smoking cessation is strongly advised because nicotine impairs perfusion and increases necrosis risk.
Revision options are available when aesthetic goals are not met. Autologous fat grafting can restore lost projection, scar revision (laser resurfacing or silicone sheets) refines texture, and additional medical tattooing sessions adjust color or shape. In some cases, a small silicone or Gore‑Tex implant is placed beneath the nipple to augment height.
Insurance coverage for nipple reconstruction and associated areola tattooing is generally provided under the Women’s Health and Cancer Rights Act of 1998, which requires U.S. health plans to cover all stages of breast reconstruction after mastectomy. Patients should verify individual policy details with their insurer and may receive assistance from the surgical practice’s billing staff.
What are the most common complications after nipple reconstruction?
Complications are rare but can include temporary numbness, infection, hematoma, or loss of projection over time. Using flap techniques that preserve vascularity and employing meticulous suturing reduce these risks.
Dr. Thomas W. Loeb’s Integrated Approach to Natural Results
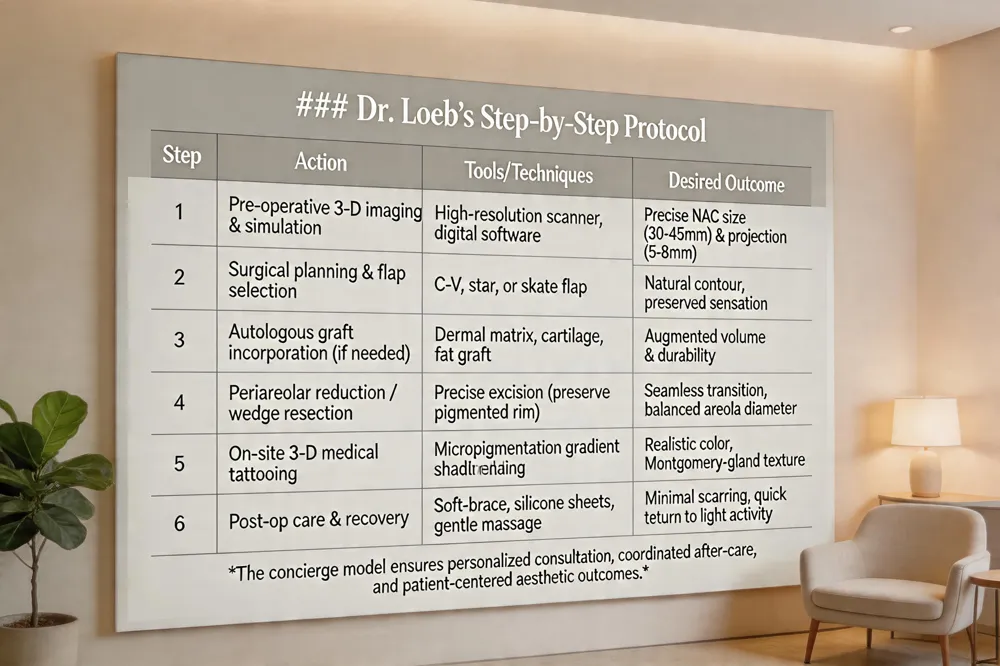 Dr. Thomas W. Loeb is a double‑board‑certified plastic surgeon (American Board of Plastic Surgery and American Board of Surgery) and an active member of the American Society of Plastic Surgeons, guaranteeing adherence to the highest safety and ethical standards. His Manhattan boutique practice blends surgical precision with cutting‑edge technology: using pre‑operative three‑dimensional imaging and digital simulation, he maps the ideal nipple‑areola complex (NAC) size, projection (5–8 mm) and areolar diameter (30–45 mm) for each patient’s unique anatomy. During surgery he employs flap techniques (C‑V, star or skate flaps), autologous grafts (dermal, cartilage, or fat) and, when needed, periareolar reduction or wedge resection to achieve natural contour while preserving neurovascular supply. After the nipple is created, Dr. Loeb offers on‑site medical tattooing—often using 3‑D micropigmentation—to match pigment, gradient shading and Montgomery‑gland texture, and can refer patients to specialist tattoo artists for customized designs. The practice’s personalized, concierge model ensures ample consultation time, tailored treatment planning and coordinated after‑care, allowing patients to resume light activity within a week and achieve a seamless, natural‑looking NAC that harmonizes with the augmented breast.
Putting It All Together for a Harmonious Breast Aesthetic
A successful breast aesthetic begins with personalized treatment planning that evaluates each patient’s anatomy, aesthetic goals, and lifestyle factors such as smoking status, prior radiation, and future breastfeeding plans. Surgeons map nipple‑areola dimensions (typically 30‑45 mm areola diameter and 4‑8 mm nipple projection) and use 3‑D imaging to visualize outcomes, ensuring proportionate results. The most natural‑looking outcomes arise from a synergistic blend of surgical and non‑surgical techniques: local flap reconstruction or autologous tissue grafts create projection, while medical tattooing (including 3‑D micropigmentation) restores realistic color and shading. Adjunctive options—injectable hyaluronic‑acid fillers for temporary projection, fat grafting for tissue thickness, or silicone prosthetics for non‑surgical patients—fine‑tune the final look without compromising safety. Selecting a board‑certified plastic surgeon with dedicated NAC expertise guarantees adherence to evidence‑based protocols, meticulous neurovascular preservation, and comprehensive after‑care, delivering lasting, natural results that enhance both form and function.
Why Natural‑Looking Nipple & Areola Enhancement Matters
Patients seeking breast augmentation or reconstruction expect a result that looks and feels like their own tissue; the nipple‑areola complex (NAC) is the visual focal point that determines whether the breast appears natural or prosthetic. A proportionate areola (30–45 mm) with a subtle darker rim and a nipple projection of 4–8 mm creates harmonious balance and preserves the illusion of normal anatomy. Achieving this balance requires a tailored mix of surgical and non‑surgical options. Surgical techniques—such as periareolar excision for areola reduction, local flap reconstruction (C‑V, star, or donut flaps) for nipple projection, and autologous grafts—address size, shape, and texture while maintaining neurovascular integrity. Non‑surgical adjuncts, including 3‑D medical tattooing, hyaluronic‑acid fillers, and nipple prosthetics, fine‑tune color, shading, and temporary projection without additional incisions. Selecting the appropriate combination, guided by board‑certified surgeons, ensures realistic aesthetics, optimal healing, and lasting patient satisfaction.
Surgical Foundations: Flaps, Grafts, and Reduction Techniques
 Local flap designs remain the cornerstone for achieving a natural‑looking nipple projection. The C‑V, star, skate, and donut flaps use the patient’s own breast skin, preserving the neurovascular bundle and tactile sensation while creating a three‑dimensional nipple. When tissue quality is compromised—such as after radiation or in very thin breasts—autologous grafts (fat, dermal matrix, or cartilage) can be incorporated into the flap core to augment volume and prolong projection.
For hypertrophic nipples or oversized areolas, periareolar excision, wedge resection, and circumferential reduction techniques remove excess skin and pigment while maintaining the pigmented rim for a seamless transition. These procedures are performed through a single, well‑placed incision that minimizes scarring and protects blood flow.
Preserving neurovascular supply is essential; surgeons avoid full‑thickness circumferential incisions and use meticulous suturing to maintain perfusion and sensation.
Answer to the question: Local skin flaps—particularly the C‑V, star, and donut designs—provide the most natural nipple projection because they use the patient’s native tissue and retain sensation. Adding autologous fat grafts or cartilage grafts can further enhance durability, especially in radiated or thin tissue.
Non‑Surgical Enhancements: Medical Tattooing, Fillers, and Prosthetics
 Medical‑grade 3‑D tattooing (micropigmentation) is now a standard, minimally invasive option for recreating the color, shading and texture of the nipple‑areola complex. Advanced 3‑D techniques blend a darker central nipple hue with a lighter peripheral rim, producing a realistic three‑dimensional illusion in a single session and offering a broad palette that matches the patient’s natural skin tone.
Hyaluronic‑acid fillers such as Juvéderm or Restylane can be injected beneath the nipple to add temporary projection. The procedure is performed with a fine needle in an office setting, usually requiring only one syringe per side and allowing patients to resume normal activities within 1–2 days. Projection gains last several years, but the filler does not provide permanent support and may disrupt ductal architecture, so surgeons advise deferring treatment until childbearing is complete and breastfeeding is no longer planned.
Nipple prosthetics provide a removable, non‑surgical alternative for patients who prefer not to undergo surgery or tattooing. Modern prosthetics mimic the look and feel of a natural nipple and can be fitted to the breast mound after reconstruction or augmentation.
Can injectable fillers replace surgery for nipple projection? Injectable hyaluronic‑acid fillers can increase nipple height for a few years with a quick, office‑based procedure, yet they are temporary, may affect ductal structures, and are generally not recommended for women planning future pregnancy or breastfeeding. Surgical options remain the definitive solution for lasting projection.
Timing, Eligibility, and Patient‑Specific Factors
 Nipple reconstruction is most successful when performed after the breast mound has stabilized. In practice, surgeons schedule the procedure 3–4 months after tissue‑sparing mastectomy or autologous flap reconstruction, allowing postoperative edema to resolve and incisional healing to mature. For implant‑based reconstruction, a slightly longer interval of 4–6 months is common to ensure the implant position is permanent before local flaps or grafts are created.
Eligibility for nipple‑sparing mastectomy (NSM) is limited by oncologic factors. Patients with inflammatory breast cancer, tumors involving the nipple‑areola complex, or cancer‑related nipple discharge are excluded because preserving the NAC could leave residual disease. Likewise, active infection or uncontrolled systemic illness contraindicates NSM.
Patient‑specific variables strongly influence outcomes. Prior radiation therapy compromises skin elasticity and vascularity, increasing the risk of nipple necrosis or loss of projection. Smoking diminishes microcirculation and impairs wound healing, while dense scar tissue or a thinned skin envelope can limit flap viability. Pre‑operative assessment should therefore include a detailed history of radiation, smoking status, and scar quality.
Modern planning tools mitigate these risks. High‑resolution 3‑D imaging and digital simulation allow the surgeon to visualize the final nipple‑areola complex, predict symmetry, and customize flap dimensions. Such personalized planning improves aesthetic predictability and helps set realistic patient expectations.
When is the optimal window for nipple reconstruction? Most surgeons schedule nipple reconstruction 3‑4 months after the breast mound is created, allowing swelling to subside and tissue to heal. For implant‑based reconstruction, a 4‑6 month interval is common to ensure stable positioning before flap or graft work.
Managing Risks, Recovery, and Long‑Term Aesthetic Refinement
 Nipple reconstruction, whether performed with local skin flaps, grafts, or medical tattooing, carries a low but meaningful complication profile. The most common issues include infection, hematoma, temporary numbness, partial or total necrosis of the reconstructed nipple, loss of projection (often 50‑60 % within two years), and pigment irregularities such as fading or uneven color match. Meticulous flap design that preserves neurovascular supply, gentle handling of tissue, and prophylactic antibiotics help mitigate these risks.
Post‑operative care is essential for optimal healing. Patients are instructed to keep the nipple‑areola complex protected from friction, wear a soft, non‑underwired bra after dressing removal, and apply silicone gel sheets to the scar to improve texture. Gentle massage of the surrounding breast tissue promotes circulation, while smoking cessation is strongly advised because nicotine impairs perfusion and increases necrosis risk.
Revision options are available when aesthetic goals are not met. Autologous fat grafting can restore lost projection, scar revision (laser resurfacing or silicone sheets) refines texture, and additional medical tattooing sessions adjust color or shape. In some cases, a small silicone or Gore‑Tex implant is placed beneath the nipple to augment height.
Insurance coverage for nipple reconstruction and associated areola tattooing is generally provided under the Women’s Health and Cancer Rights Act of 1998, which requires U.S. health plans to cover all stages of breast reconstruction after mastectomy. Patients should verify individual policy details with their insurer and may receive assistance from the surgical practice’s billing staff.
What are the most common complications after nipple reconstruction?
Complications are rare but can include temporary numbness, infection, hematoma, or loss of projection over time. Using flap techniques that preserve vascularity and employing meticulous suturing reduce these risks.
Dr. Thomas W. Loeb’s Integrated Approach to Natural Results
 Dr. Thomas W. Loeb is a double‑board‑certified plastic surgeon (American Board of Plastic Surgery and American Board of Surgery) and an active member of the American Society of Plastic Surgeons, guaranteeing adherence to the highest safety and ethical standards. His Manhattan boutique practice blends surgical precision with cutting‑edge technology: using pre‑operative three‑dimensional imaging and digital simulation, he maps the ideal nipple‑areola complex (NAC) size, projection (5–8 mm) and areolar diameter (30–45 mm) for each patient’s unique anatomy. During surgery he employs flap techniques (C‑V, star or skate flaps), autologous grafts (dermal, cartilage, or fat) and, when needed, periareolar reduction or wedge resection to achieve natural contour while preserving neurovascular supply. After the nipple is created, Dr. Loeb offers on‑site medical tattooing—often using 3‑D micropigmentation—to match pigment, gradient shading and Montgomery‑gland texture, and can refer patients to specialist tattoo artists for customized designs. The practice’s personalized, concierge model ensures ample consultation time, tailored treatment planning and coordinated after‑care, allowing patients to resume light activity within a week and achieve a seamless, natural‑looking NAC that harmonizes with the augmented breast.
Putting It All Together for a Harmonious Breast Aesthetic
A successful breast aesthetic begins with personalized treatment planning that evaluates each patient’s anatomy, aesthetic goals, and lifestyle factors such as smoking status, prior radiation, and future breastfeeding plans. Surgeons map nipple‑areola dimensions (typically 30‑45 mm areola diameter and 4‑8 mm nipple projection) and use 3‑D imaging to visualize outcomes, ensuring proportionate results. The most natural‑looking outcomes arise from a synergistic blend of surgical and non‑surgical techniques: local flap reconstruction or autologous tissue grafts create projection, while medical tattooing (including 3‑D micropigmentation) restores realistic color and shading. Adjunctive options—injectable hyaluronic‑acid fillers for temporary projection, fat grafting for tissue thickness, or silicone prosthetics for non‑surgical patients—fine‑tune the final look without compromising safety. Selecting a board‑certified plastic surgeon with dedicated NAC expertise guarantees adherence to evidence‑based protocols, meticulous neurovascular preservation, and comprehensive after‑care, delivering lasting, natural results that enhance both form and function.
Heading
Why Natural‑Looking Nipple & Areola Enhancement Matters
Patients seeking breast augmentation or reconstruction expect a result that looks and feels like their own tissue; the nipple‑areola complex (NAC) is the visual focal point that determines whether the breast appears natural or prosthetic. A proportionate areola (30–45 mm) with a subtle darker rim and a nipple projection of 4–8 mm creates harmonious balance and preserves the illusion of normal anatomy. Achieving this balance requires a tailored mix of surgical and non‑surgical options. Surgical techniques—such as periareolar excision for areola reduction, local flap reconstruction (C‑V, star, or donut flaps) for nipple projection, and autologous grafts—address size, shape, and texture while maintaining neurovascular integrity. Non‑surgical adjuncts, including 3‑D medical tattooing, hyaluronic‑acid fillers, and nipple prosthetics, fine‑tune color, shading, and temporary projection without additional incisions. Selecting the appropriate combination, guided by board‑certified surgeons, ensures realistic aesthetics, optimal healing, and lasting patient satisfaction.
Surgical Foundations: Flaps, Grafts, and Reduction Techniques
 Local flap designs remain the cornerstone for achieving a natural‑looking nipple projection. The C‑V, star, skate, and donut flaps use the patient’s own breast skin, preserving the neurovascular bundle and tactile sensation while creating a three‑dimensional nipple. When tissue quality is compromised—such as after radiation or in very thin breasts—autologous grafts (fat, dermal matrix, or cartilage) can be incorporated into the flap core to augment volume and prolong projection.
For hypertrophic nipples or oversized areolas, periareolar excision, wedge resection, and circumferential reduction techniques remove excess skin and pigment while maintaining the pigmented rim for a seamless transition. These procedures are performed through a single, well‑placed incision that minimizes scarring and protects blood flow.
Preserving neurovascular supply is essential; surgeons avoid full‑thickness circumferential incisions and use meticulous suturing to maintain perfusion and sensation.
Answer to the question: Local skin flaps—particularly the C‑V, star, and donut designs—provide the most natural nipple projection because they use the patient’s native tissue and retain sensation. Adding autologous fat grafts or cartilage grafts can further enhance durability, especially in radiated or thin tissue.
Non‑Surgical Enhancements: Medical Tattooing, Fillers, and Prosthetics
 Medical‑grade 3‑D tattooing (micropigmentation) is now a standard, minimally invasive option for recreating the color, shading and texture of the nipple‑areola complex. Advanced 3‑D techniques blend a darker central nipple hue with a lighter peripheral rim, producing a realistic three‑dimensional illusion in a single session and offering a broad palette that matches the patient’s natural skin tone.
Hyaluronic‑acid fillers such as Juvéderm or Restylane can be injected beneath the nipple to add temporary projection. The procedure is performed with a fine needle in an office setting, usually requiring only one syringe per side and allowing patients to resume normal activities within 1–2 days. Projection gains last several years, but the filler does not provide permanent support and may disrupt ductal architecture, so surgeons advise deferring treatment until childbearing is complete and breastfeeding is no longer planned.
Nipple prosthetics provide a removable, non‑surgical alternative for patients who prefer not to undergo surgery or tattooing. Modern prosthetics mimic the look and feel of a natural nipple and can be fitted to the breast mound after reconstruction or augmentation.
Can injectable fillers replace surgery for nipple projection? Injectable hyaluronic‑acid fillers can increase nipple height for a few years with a quick, office‑based procedure, yet they are temporary, may affect ductal structures, and are generally not recommended for women planning future pregnancy or breastfeeding. Surgical options remain the definitive solution for lasting projection.
Timing, Eligibility, and Patient‑Specific Factors
 Nipple reconstruction is most successful when performed after the breast mound has stabilized. In practice, surgeons schedule the procedure 3–4 months after tissue‑sparing mastectomy or autologous flap reconstruction, allowing postoperative edema to resolve and incisional healing to mature. For implant‑based reconstruction, a slightly longer interval of 4–6 months is common to ensure the implant position is permanent before local flaps or grafts are created.
Eligibility for nipple‑sparing mastectomy (NSM) is limited by oncologic factors. Patients with inflammatory breast cancer, tumors involving the nipple‑areola complex, or cancer‑related nipple discharge are excluded because preserving the NAC could leave residual disease. Likewise, active infection or uncontrolled systemic illness contraindicates NSM.
Patient‑specific variables strongly influence outcomes. Prior radiation therapy compromises skin elasticity and vascularity, increasing the risk of nipple necrosis or loss of projection. Smoking diminishes microcirculation and impairs wound healing, while dense scar tissue or a thinned skin envelope can limit flap viability. Pre‑operative assessment should therefore include a detailed history of radiation, smoking status, and scar quality.
Modern planning tools mitigate these risks. High‑resolution 3‑D imaging and digital simulation allow the surgeon to visualize the final nipple‑areola complex, predict symmetry, and customize flap dimensions. Such personalized planning improves aesthetic predictability and helps set realistic patient expectations.
When is the optimal window for nipple reconstruction? Most surgeons schedule nipple reconstruction 3‑4 months after the breast mound is created, allowing swelling to subside and tissue to heal. For implant‑based reconstruction, a 4‑6 month interval is common to ensure stable positioning before flap or graft work.
Managing Risks, Recovery, and Long‑Term Aesthetic Refinement
 Nipple reconstruction, whether performed with local skin flaps, grafts, or medical tattooing, carries a low but meaningful complication profile. The most common issues include infection, hematoma, temporary numbness, partial or total necrosis of the reconstructed nipple, loss of projection (often 50‑60 % within two years), and pigment irregularities such as fading or uneven color match. Meticulous flap design that preserves neurovascular supply, gentle handling of tissue, and prophylactic antibiotics help mitigate these risks.
Post‑operative care is essential for optimal healing. Patients are instructed to keep the nipple‑areola complex protected from friction, wear a soft, non‑underwired bra after dressing removal, and apply silicone gel sheets to the scar to improve texture. Gentle massage of the surrounding breast tissue promotes circulation, while smoking cessation is strongly advised because nicotine impairs perfusion and increases necrosis risk.
Revision options are available when aesthetic goals are not met. Autologous fat grafting can restore lost projection, scar revision (laser resurfacing or silicone sheets) refines texture, and additional medical tattooing sessions adjust color or shape. In some cases, a small silicone or Gore‑Tex implant is placed beneath the nipple to augment height.
Insurance coverage for nipple reconstruction and associated areola tattooing is generally provided under the Women’s Health and Cancer Rights Act of 1998, which requires U.S. health plans to cover all stages of breast reconstruction after mastectomy. Patients should verify individual policy details with their insurer and may receive assistance from the surgical practice’s billing staff.
What are the most common complications after nipple reconstruction?
Complications are rare but can include temporary numbness, infection, hematoma, or loss of projection over time. Using flap techniques that preserve vascularity and employing meticulous suturing reduce these risks.
Dr. Thomas W. Loeb’s Integrated Approach to Natural Results
 Dr. Thomas W. Loeb is a double‑board‑certified plastic surgeon (American Board of Plastic Surgery and American Board of Surgery) and an active member of the American Society of Plastic Surgeons, guaranteeing adherence to the highest safety and ethical standards. His Manhattan boutique practice blends surgical precision with cutting‑edge technology: using pre‑operative three‑dimensional imaging and digital simulation, he maps the ideal nipple‑areola complex (NAC) size, projection (5–8 mm) and areolar diameter (30–45 mm) for each patient’s unique anatomy. During surgery he employs flap techniques (C‑V, star or skate flaps), autologous grafts (dermal, cartilage, or fat) and, when needed, periareolar reduction or wedge resection to achieve natural contour while preserving neurovascular supply. After the nipple is created, Dr. Loeb offers on‑site medical tattooing—often using 3‑D micropigmentation—to match pigment, gradient shading and Montgomery‑gland texture, and can refer patients to specialist tattoo artists for customized designs. The practice’s personalized, concierge model ensures ample consultation time, tailored treatment planning and coordinated after‑care, allowing patients to resume light activity within a week and achieve a seamless, natural‑looking NAC that harmonizes with the augmented breast.
Putting It All Together for a Harmonious Breast Aesthetic
A successful breast aesthetic begins with personalized treatment planning that evaluates each patient’s anatomy, aesthetic goals, and lifestyle factors such as smoking status, prior radiation, and future breastfeeding plans. Surgeons map nipple‑areola dimensions (typically 30‑45 mm areola diameter and 4‑8 mm nipple projection) and use 3‑D imaging to visualize outcomes, ensuring proportionate results. The most natural‑looking outcomes arise from a synergistic blend of surgical and non‑surgical techniques: local flap reconstruction or autologous tissue grafts create projection, while medical tattooing (including 3‑D micropigmentation) restores realistic color and shading. Adjunctive options—injectable hyaluronic‑acid fillers for temporary projection, fat grafting for tissue thickness, or silicone prosthetics for non‑surgical patients—fine‑tune the final look without compromising safety. Selecting a board‑certified plastic surgeon with dedicated NAC expertise guarantees adherence to evidence‑based protocols, meticulous neurovascular preservation, and comprehensive after‑care, delivering lasting, natural results that enhance both form and function.





Locations


© 2014 - 2025. Thomas W. Loeb | Board Certified Plastic Surgeon