.png)


.svg)
.svg)

Rebuilding Confidence: Nipple Reconstruction After Mastectomy
News
/
April 22, 2026
Nipple Reconstruction After Mastectomy: Options and Outcomes
Rebuilding Confidence: Nipple Reconstruction After Mastectomy

Body contouring has revolutionized the way we think about self-care and aesthetic transformations. It’s more than just a cosmetic procedure—it’s a path to enhanced confidence and self-expression.
Understanding the Journey
Restoring the nipple‑areola complex (NAC) after mastectomy is a key step in achieving body‑image confidence and psychosocial well‑being; patients report higher satisfaction, improved self‑esteem, and a sense of wholeness when a natural‑looking NAC is recreated. Nipple‑sparing mastectomy (NSM) is oncologically safe for carefully selected candidates—early‑stage, small, peripheral tumors at least 2 cm from the nipple—showing low loco‑regional recurrence rates comparable to total mastectomy (≈4 %). After the primary breast mound (implant or flap) has healed and the skin envelope stabilises, nipple‑areola reconstruction is typically performed 3–6 months post‑reconstruction, allowing adequate tissue recovery and minimizing complications. This timing aligns with recommendations from the American Cancer Society and plastic‑surgery guidelines.
Surgical Techniques for Nipple Creation

Nipple reconstruction after mastectomy most most often performed with local skin‑flap methods. The C‑V flap, star flap, skate flap, and mushroom flap each use a small piece of skin from the reconstructed breast, reshaped and sutured to produce a projecting nipple; these outpatient procedures typically last 15‑60 minutes and rely on the patient’s own tissue for a natural feel. When local skin is insufficient, skin‑graft or dermal‑graft options are employed, using full‑thickness grafts from donor sites (inner thigh, abdomen, buttock) or autologous dermal tissue to form the areola and augment projection. Composite grafts—often combining cartilage or synthetic cores with flap tissue—provide added durability, especially in thin or irradiated skin, and help preserve height over time. An investigational alternative is the collagen‑elastin NAC graft, a scaffold derived from donor nipple‑areolar tissue that can be stored and later stitched onto a reconstructed breast. Unlike traditional flaps, the graft offers a pre‑shaped, lifelike nipple and areola that integrates with the patient’s own cells within two to three weeks, eliminating the need for extensive flap sculpting and potentially reducing projection loss. These techniques, combined with subsequent medical tattooing for areolar pigmentation, aim to restore symmetry, color match, and projection, enhancing aesthetic satisfaction and psychosocial well‑being after breast reconstruction.
Implant‑Based Reconstruction & Nipple‑Sparing Mastectomy

Nipple‑sparing mastectomy (NSM) preserves the native nipple‑areolar complex (NAC) in 90‑95 % of carefully selected patients, making it an attractive partner for implant‑based breast reconstruction (IBBR). Because the skin envelope remains intact, surgeons can perform immediate IBBR in roughly 80 % of cases, offering superior cosmetic and psychosocial outcomes compared with total mastectomy (TM) or skin‑sparing mastectomy (SSM) that later require nipple reconstruction. However, adding NSM to IBBR raises overall complication rates to about 20‑30 % (vs. 8‑10 % after TM + IBBR), driven mainly by skin‑flap ischemia (4‑20 %) and higher incidences of infection (1.5‑9 %).
Meta‑analyses of these approaches show no statistically significant difference in overall infection, seroma, hematoma, or capsular contracture rates. One‑stage procedures, however, exhibit modestly higher rates of flap necrosis, re‑operation, and implant loss. whereas two‑stage reconstructions may extend the overall treatment timeline but tend to reduce those specific risks.
In summary, NSM + IBBR provides excellent aesthetic results but comes with a higher complication profile, especially for flap‑related issues. The choice between one‑stage and two‑stage IBBR should balance the patient’s oncologic status, breast size, smoking history, and preferences regarding the timing and potential for additional surgeries.
Timing and Sequencing: When to Reconstruct

Incision placement during the initial mastectomy or reconstruction markedly influences necrosis risk. Laterally placed or inframammary incisions preserve the subdermal vascular network that supplies the NAC, resulting in lower rates of nipple loss. In contrast, peri‑areolar incisions disrupt this blood flow and are associated with a higher incidence of partial or complete nipple necrosis.
Thus, optimal timing balances tissue healing with oncologic treatment schedules, and careful incision planning is essential to protect NAC viability and achieve durable aesthetic outcomes.
Non‑Surgical Options: Tattooing and Prosthetics

Medical tattooing, also called micropigmentation, is used to colour the areola after mastectomy. A pigment is deposited into the dermis to match the contralateral side, providing a permanent, low‑maintenance colour match. When patients elect to for surgical nipple creation, three‑dimensional (3‑D) medical tattooing can simulate both nipple projection and areola colour. By applying layered shading and pigment depth, the technique creates the illusion of a raised nipple on a flat surface, healing within 7‑10 days, but it does not restore tactile sensation or true projection. Silicone prosthetic nipples and adhesive options offer a removable, non‑surgical alternative. These prostheses can be colour‑matched, attached to the chest, and removed for hygiene or personal preference, making them suitable for patients with compromised skin, those who wish to avoid additional surgery, or anyone desiring a flexible aesthetic solution.
What does 3‑D medical tattooing achieve for patients who skip surgical nipple creation?
3‑D tattooing uses shading and pigment depth to simulate nipple projection and areola colour on a flat surface. While it offers a realistic appearance and heals in 7‑10 days, it does not provide actual projection or tactile sensation.
When might a patient choose a silicone prosthetic nipple over surgery?
Prosthetic nipples are ideal for patients who wish to avoid additional surgery, have compromised skin quality, or prefer a removable solution. They can be attached to the chest and matched to the contralateral side in colour and size, providing an aesthetic result without surgical risk.
Complications, Risks, and Managing Expectations

Implant‑based reconstruction after nipple‑sparing mastectomy carries predictable complications. Complication rates after NSM + IBBR range from 1.5 % to 9 % for surgical‑site infection, 1 %–5 % for seroma requiring treatment, 1 %–3 % for hematoma, 4 %–20 % for skin‑flap ischemia, and 3 %–12 % for necrosis; nipple necrosis leading to loss occurs in 1 %–5 % of cases. Smoking and prior radiation markedly increase these risks: active smokers experience a three‑fold rise in flap necrosis and infection, while irradiated fields raise infection to ≈20 % and implant loss to 5‑15 %. Obesity (BMI ≥ 30) doubles the risk of peri‑operative complications and increases reconstructive failure risk seven‑fold in implant‑based reconstruction. A rare but serious concern is breast‑implant‑associated anaplastic large‑cell lymphoma (BIA‑ALCL) is a rare but recognized risk, predominantly linked to textured implants; patients should be counseled on this risk and offered smooth‑surface options when appropriate.
Patient Satisfaction, Quality of Life, and Future Innovations
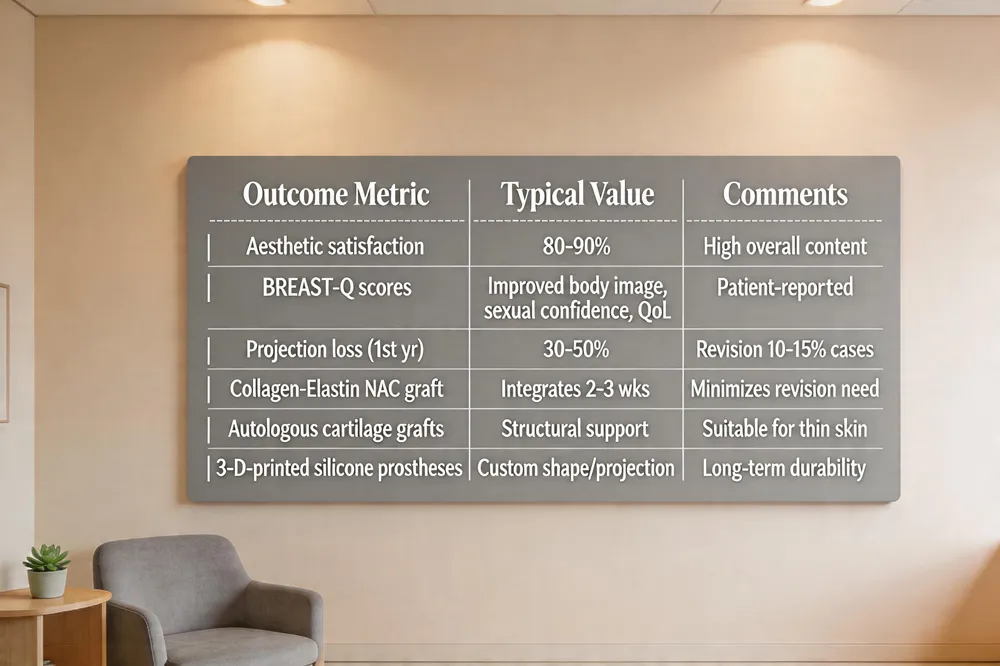
Patient-reported outcomes after nipple reconstruction are overwhelmingly positive; 80‑90 % of women rate their aesthetic result as satisfactory and BREAST‑Q scores consistently show marked improvements in body image, sexual confidence, and overall quality of life. The most common long‑term issue is loss of nipple projection, typically 30‑50 % within the first year, leading to revision surgery in about 10‑15 % of cases. Emerging technologies aim to mitigate this. The collagen‑elastin NAC graft, developed by Dr. Pashos, integrates within weeks and provides a natural‑looking, durable nipple‑areola complex. Autologous cartilage grafts and 3‑D‑printed silicone prostheses also promise sustained projection and reduced need for secondary revisions, expanding the reconstructive armamentarium.
The Final Piece of the Reconstruction Puzzle
After the breast mound is healed, the last step in a reconstruction journey is nipple‑areola restoration. Options include local flap reconstruction (C‑V, star, skate), skin grafts, autologous cartilage or dermal grafts, 3‑D medical tattooing, and silicone prosthetic nipples. Flap‑based techniques give physical projection but lose 30‑50 % of height within the first year; tattooing adds realistic color and can be combined for optimal symmetry. Complication rates are low—infection under 5 % and necrosis under 5 %—but smoking, radiation, or chemotherapy increase risk. At Dr. Loeb’s New York practice, individualized plans integrate oncologic safety, implant‑based or autologous reconstruction, and aesthetic goals. Patients are encouraged to meet a board‑certified plastic surgeon to discuss timing, preferred technique, and expected outcomes and long‑term satisfaction for each patient.
Understanding the Journey
Restoring the nipple‑areola complex (NAC) after mastectomy is a key step in achieving body‑image confidence and psychosocial well‑being; patients report higher satisfaction, improved self‑esteem, and a sense of wholeness when a natural‑looking NAC is recreated. Nipple‑sparing mastectomy (NSM) is oncologically safe for carefully selected candidates—early‑stage, small, peripheral tumors at least 2 cm from the nipple—showing low loco‑regional recurrence rates comparable to total mastectomy (≈4 %). After the primary breast mound (implant or flap) has healed and the skin envelope stabilises, nipple‑areola reconstruction is typically performed 3–6 months post‑reconstruction, allowing adequate tissue recovery and minimizing complications. This timing aligns with recommendations from the American Cancer Society and plastic‑surgery guidelines.
Surgical Techniques for Nipple Creation
Nipple reconstruction after mastectomy most most often performed with local skin‑flap methods. The C‑V flap, star flap, skate flap, and mushroom flap each use a small piece of skin from the reconstructed breast, reshaped and sutured to produce a projecting nipple; these outpatient procedures typically last 15‑60 minutes and rely on the patient’s own tissue for a natural feel. When local skin is insufficient, skin‑graft or dermal‑graft options are employed, using full‑thickness grafts from donor sites (inner thigh, abdomen, buttock) or autologous dermal tissue to form the areola and augment projection. Composite grafts—often combining cartilage or synthetic cores with flap tissue—provide added durability, especially in thin or irradiated skin, and help preserve height over time. An investigational alternative is the collagen‑elastin NAC graft, a scaffold derived from donor nipple‑areolar tissue that can be stored and later stitched onto a reconstructed breast. Unlike traditional flaps, the graft offers a pre‑shaped, lifelike nipple and areola that integrates with the patient’s own cells within two to three weeks, eliminating the need for extensive flap sculpting and potentially reducing projection loss. These techniques, combined with subsequent medical tattooing for areolar pigmentation, aim to restore symmetry, color match, and projection, enhancing aesthetic satisfaction and psychosocial well‑being after breast reconstruction.
Implant‑Based Reconstruction & Nipple‑Sparing Mastectomy
Nipple‑sparing mastectomy (NSM) preserves the native nipple‑areolar complex (NAC) in 90‑95 % of carefully selected patients, making it an attractive partner for implant‑based breast reconstruction (IBBR). Because the skin envelope remains intact, surgeons can perform immediate IBBR in roughly 80 % of cases, offering superior cosmetic and psychosocial outcomes compared with total mastectomy (TM) or skin‑sparing mastectomy (SSM) that later require nipple reconstruction. However, adding NSM to IBBR raises overall complication rates to about 20‑30 % (vs. 8‑10 % after TM + IBBR), driven mainly by skin‑flap ischemia (4‑20 %) and higher incidences of infection (1.5‑9 %).
Meta‑analyses of these approaches show no statistically significant difference in overall infection, seroma, hematoma, or capsular contracture rates. One‑stage procedures, however, exhibit modestly higher rates of flap necrosis, re‑operation, and implant loss. whereas two‑stage reconstructions may extend the overall treatment timeline but tend to reduce those specific risks.
In summary, NSM + IBBR provides excellent aesthetic results but comes with a higher complication profile, especially for flap‑related issues. The choice between one‑stage and two‑stage IBBR should balance the patient’s oncologic status, breast size, smoking history, and preferences regarding the timing and potential for additional surgeries.
Timing and Sequencing: When to Reconstruct
Incision placement during the initial mastectomy or reconstruction markedly influences necrosis risk. Laterally placed or inframammary incisions preserve the subdermal vascular network that supplies the NAC, resulting in lower rates of nipple loss. In contrast, peri‑areolar incisions disrupt this blood flow and are associated with a higher incidence of partial or complete nipple necrosis.
Thus, optimal timing balances tissue healing with oncologic treatment schedules, and careful incision planning is essential to protect NAC viability and achieve durable aesthetic outcomes.
Non‑Surgical Options: Tattooing and Prosthetics
Medical tattooing, also called micropigmentation, is used to colour the areola after mastectomy. A pigment is deposited into the dermis to match the contralateral side, providing a permanent, low‑maintenance colour match. When patients elect to for surgical nipple creation, three‑dimensional (3‑D) medical tattooing can simulate both nipple projection and areola colour. By applying layered shading and pigment depth, the technique creates the illusion of a raised nipple on a flat surface, healing within 7‑10 days, but it does not restore tactile sensation or true projection. Silicone prosthetic nipples and adhesive options offer a removable, non‑surgical alternative. These prostheses can be colour‑matched, attached to the chest, and removed for hygiene or personal preference, making them suitable for patients with compromised skin, those who wish to avoid additional surgery, or anyone desiring a flexible aesthetic solution.
What does 3‑D medical tattooing achieve for patients who skip surgical nipple creation?
3‑D tattooing uses shading and pigment depth to simulate nipple projection and areola colour on a flat surface. While it offers a realistic appearance and heals in 7‑10 days, it does not provide actual projection or tactile sensation.
When might a patient choose a silicone prosthetic nipple over surgery?
Prosthetic nipples are ideal for patients who wish to avoid additional surgery, have compromised skin quality, or prefer a removable solution. They can be attached to the chest and matched to the contralateral side in colour and size, providing an aesthetic result without surgical risk.
Complications, Risks, and Managing Expectations
Implant‑based reconstruction after nipple‑sparing mastectomy carries predictable complications. Complication rates after NSM + IBBR range from 1.5 % to 9 % for surgical‑site infection, 1 %–5 % for seroma requiring treatment, 1 %–3 % for hematoma, 4 %–20 % for skin‑flap ischemia, and 3 %–12 % for necrosis; nipple necrosis leading to loss occurs in 1 %–5 % of cases. Smoking and prior radiation markedly increase these risks: active smokers experience a three‑fold rise in flap necrosis and infection, while irradiated fields raise infection to ≈20 % and implant loss to 5‑15 %. Obesity (BMI ≥ 30) doubles the risk of peri‑operative complications and increases reconstructive failure risk seven‑fold in implant‑based reconstruction. A rare but serious concern is breast‑implant‑associated anaplastic large‑cell lymphoma (BIA‑ALCL) is a rare but recognized risk, predominantly linked to textured implants; patients should be counseled on this risk and offered smooth‑surface options when appropriate.
Patient Satisfaction, Quality of Life, and Future Innovations
Patient-reported outcomes after nipple reconstruction are overwhelmingly positive; 80‑90 % of women rate their aesthetic result as satisfactory and BREAST‑Q scores consistently show marked improvements in body image, sexual confidence, and overall quality of life. The most common long‑term issue is loss of nipple projection, typically 30‑50 % within the first year, leading to revision surgery in about 10‑15 % of cases. Emerging technologies aim to mitigate this. The collagen‑elastin NAC graft, developed by Dr. Pashos, integrates within weeks and provides a natural‑looking, durable nipple‑areola complex. Autologous cartilage grafts and 3‑D‑printed silicone prostheses also promise sustained projection and reduced need for secondary revisions, expanding the reconstructive armamentarium.
The Final Piece of the Reconstruction Puzzle
After the breast mound is healed, the last step in a reconstruction journey is nipple‑areola restoration. Options include local flap reconstruction (C‑V, star, skate), skin grafts, autologous cartilage or dermal grafts, 3‑D medical tattooing, and silicone prosthetic nipples. Flap‑based techniques give physical projection but lose 30‑50 % of height within the first year; tattooing adds realistic color and can be combined for optimal symmetry. Complication rates are low—infection under 5 % and necrosis under 5 %—but smoking, radiation, or chemotherapy increase risk. At Dr. Loeb’s New York practice, individualized plans integrate oncologic safety, implant‑based or autologous reconstruction, and aesthetic goals. Patients are encouraged to meet a board‑certified plastic surgeon to discuss timing, preferred technique, and expected outcomes and long‑term satisfaction for each patient.
Heading
Understanding the Journey
Restoring the nipple‑areola complex (NAC) after mastectomy is a key step in achieving body‑image confidence and psychosocial well‑being; patients report higher satisfaction, improved self‑esteem, and a sense of wholeness when a natural‑looking NAC is recreated. Nipple‑sparing mastectomy (NSM) is oncologically safe for carefully selected candidates—early‑stage, small, peripheral tumors at least 2 cm from the nipple—showing low loco‑regional recurrence rates comparable to total mastectomy (≈4 %). After the primary breast mound (implant or flap) has healed and the skin envelope stabilises, nipple‑areola reconstruction is typically performed 3–6 months post‑reconstruction, allowing adequate tissue recovery and minimizing complications. This timing aligns with recommendations from the American Cancer Society and plastic‑surgery guidelines.
Surgical Techniques for Nipple Creation
Nipple reconstruction after mastectomy most most often performed with local skin‑flap methods. The C‑V flap, star flap, skate flap, and mushroom flap each use a small piece of skin from the reconstructed breast, reshaped and sutured to produce a projecting nipple; these outpatient procedures typically last 15‑60 minutes and rely on the patient’s own tissue for a natural feel. When local skin is insufficient, skin‑graft or dermal‑graft options are employed, using full‑thickness grafts from donor sites (inner thigh, abdomen, buttock) or autologous dermal tissue to form the areola and augment projection. Composite grafts—often combining cartilage or synthetic cores with flap tissue—provide added durability, especially in thin or irradiated skin, and help preserve height over time. An investigational alternative is the collagen‑elastin NAC graft, a scaffold derived from donor nipple‑areolar tissue that can be stored and later stitched onto a reconstructed breast. Unlike traditional flaps, the graft offers a pre‑shaped, lifelike nipple and areola that integrates with the patient’s own cells within two to three weeks, eliminating the need for extensive flap sculpting and potentially reducing projection loss. These techniques, combined with subsequent medical tattooing for areolar pigmentation, aim to restore symmetry, color match, and projection, enhancing aesthetic satisfaction and psychosocial well‑being after breast reconstruction.
Implant‑Based Reconstruction & Nipple‑Sparing Mastectomy
Nipple‑sparing mastectomy (NSM) preserves the native nipple‑areolar complex (NAC) in 90‑95 % of carefully selected patients, making it an attractive partner for implant‑based breast reconstruction (IBBR). Because the skin envelope remains intact, surgeons can perform immediate IBBR in roughly 80 % of cases, offering superior cosmetic and psychosocial outcomes compared with total mastectomy (TM) or skin‑sparing mastectomy (SSM) that later require nipple reconstruction. However, adding NSM to IBBR raises overall complication rates to about 20‑30 % (vs. 8‑10 % after TM + IBBR), driven mainly by skin‑flap ischemia (4‑20 %) and higher incidences of infection (1.5‑9 %).
Meta‑analyses of these approaches show no statistically significant difference in overall infection, seroma, hematoma, or capsular contracture rates. One‑stage procedures, however, exhibit modestly higher rates of flap necrosis, re‑operation, and implant loss. whereas two‑stage reconstructions may extend the overall treatment timeline but tend to reduce those specific risks.
In summary, NSM + IBBR provides excellent aesthetic results but comes with a higher complication profile, especially for flap‑related issues. The choice between one‑stage and two‑stage IBBR should balance the patient’s oncologic status, breast size, smoking history, and preferences regarding the timing and potential for additional surgeries.
Timing and Sequencing: When to Reconstruct
Incision placement during the initial mastectomy or reconstruction markedly influences necrosis risk. Laterally placed or inframammary incisions preserve the subdermal vascular network that supplies the NAC, resulting in lower rates of nipple loss. In contrast, peri‑areolar incisions disrupt this blood flow and are associated with a higher incidence of partial or complete nipple necrosis.
Thus, optimal timing balances tissue healing with oncologic treatment schedules, and careful incision planning is essential to protect NAC viability and achieve durable aesthetic outcomes.
Non‑Surgical Options: Tattooing and Prosthetics
Medical tattooing, also called micropigmentation, is used to colour the areola after mastectomy. A pigment is deposited into the dermis to match the contralateral side, providing a permanent, low‑maintenance colour match. When patients elect to for surgical nipple creation, three‑dimensional (3‑D) medical tattooing can simulate both nipple projection and areola colour. By applying layered shading and pigment depth, the technique creates the illusion of a raised nipple on a flat surface, healing within 7‑10 days, but it does not restore tactile sensation or true projection. Silicone prosthetic nipples and adhesive options offer a removable, non‑surgical alternative. These prostheses can be colour‑matched, attached to the chest, and removed for hygiene or personal preference, making them suitable for patients with compromised skin, those who wish to avoid additional surgery, or anyone desiring a flexible aesthetic solution.
What does 3‑D medical tattooing achieve for patients who skip surgical nipple creation?
3‑D tattooing uses shading and pigment depth to simulate nipple projection and areola colour on a flat surface. While it offers a realistic appearance and heals in 7‑10 days, it does not provide actual projection or tactile sensation.
When might a patient choose a silicone prosthetic nipple over surgery?
Prosthetic nipples are ideal for patients who wish to avoid additional surgery, have compromised skin quality, or prefer a removable solution. They can be attached to the chest and matched to the contralateral side in colour and size, providing an aesthetic result without surgical risk.
Complications, Risks, and Managing Expectations
Implant‑based reconstruction after nipple‑sparing mastectomy carries predictable complications. Complication rates after NSM + IBBR range from 1.5 % to 9 % for surgical‑site infection, 1 %–5 % for seroma requiring treatment, 1 %–3 % for hematoma, 4 %–20 % for skin‑flap ischemia, and 3 %–12 % for necrosis; nipple necrosis leading to loss occurs in 1 %–5 % of cases. Smoking and prior radiation markedly increase these risks: active smokers experience a three‑fold rise in flap necrosis and infection, while irradiated fields raise infection to ≈20 % and implant loss to 5‑15 %. Obesity (BMI ≥ 30) doubles the risk of peri‑operative complications and increases reconstructive failure risk seven‑fold in implant‑based reconstruction. A rare but serious concern is breast‑implant‑associated anaplastic large‑cell lymphoma (BIA‑ALCL) is a rare but recognized risk, predominantly linked to textured implants; patients should be counseled on this risk and offered smooth‑surface options when appropriate.
Patient Satisfaction, Quality of Life, and Future Innovations
Patient-reported outcomes after nipple reconstruction are overwhelmingly positive; 80‑90 % of women rate their aesthetic result as satisfactory and BREAST‑Q scores consistently show marked improvements in body image, sexual confidence, and overall quality of life. The most common long‑term issue is loss of nipple projection, typically 30‑50 % within the first year, leading to revision surgery in about 10‑15 % of cases. Emerging technologies aim to mitigate this. The collagen‑elastin NAC graft, developed by Dr. Pashos, integrates within weeks and provides a natural‑looking, durable nipple‑areola complex. Autologous cartilage grafts and 3‑D‑printed silicone prostheses also promise sustained projection and reduced need for secondary revisions, expanding the reconstructive armamentarium.
The Final Piece of the Reconstruction Puzzle
After the breast mound is healed, the last step in a reconstruction journey is nipple‑areola restoration. Options include local flap reconstruction (C‑V, star, skate), skin grafts, autologous cartilage or dermal grafts, 3‑D medical tattooing, and silicone prosthetic nipples. Flap‑based techniques give physical projection but lose 30‑50 % of height within the first year; tattooing adds realistic color and can be combined for optimal symmetry. Complication rates are low—infection under 5 % and necrosis under 5 %—but smoking, radiation, or chemotherapy increase risk. At Dr. Loeb’s New York practice, individualized plans integrate oncologic safety, implant‑based or autologous reconstruction, and aesthetic goals. Patients are encouraged to meet a board‑certified plastic surgeon to discuss timing, preferred technique, and expected outcomes and long‑term satisfaction for each patient.





Locations


© 2014 - 2025. Thomas W. Loeb | Board Certified Plastic Surgeon